




Comparison of Two Continuous Performance Test in Patients with Schizophrenia
*Beatriz López-Luengo and Alejandro González-Andrade
Department of Psychology, University of Jaen, Europe
Submission: August 19, 2016; Published: September 01, 2016
*Corresponding author: Beatriz López-Luengo, Department of Psychology, University of Jaen, Campus Las Lagunillas s/n, 23071-Jaén, Spain.
How to cite this article: Beatriz L-L, Alejandro G-A. Comparison of Two Continuous Performance Test in Patients with Schizophrenia. Psychol Behav Sci Int J. 2016; 1(2) : 555560. DOI: 10.19080/PBSIJ.2016.01.555560
Abstract
PThe Continuous Performance Test (CPT) is one of the most widely used tests in the research of cognitive deficits in patients with schizophrenia. However, little is known about the performance differences associated with the different versions of the test. The purpose of this study was examine the differences in performance between the CPT-II and the CPT-IP in a sample of forty-five patients with schizophrenia. Five response indices are compares (d’ as a sensitivity measurement, Ln β as response bias, hit and false alarm rates, and hits reaction time). Significant differences were found in all the measurements studied. The differences in the hit and false alarm rates, along with the response bias might indicate that each CPT measures different cognitive processes. A correlation analysis between socio demographic and clinical variables, and the CPTs was also performed. A significant relationship was found between the 3 and 4 digit parts of the CPT-IP and educational level. This might mean that these tasks are influenced by educational and learning components.
Keywords: Attention; Cognitive Deficits; Cognitive Processes; Educational Level
Abbreviations: CPT: Continuos Performance Test; APA: American Psychiatric Association; Ln: logarithm; HR: Hit Rate; FAR: Rate of False Alarms; RT: Reaction Times; CPT-IP: Continuous Performance Test -Identical Pairs; PANSS: Positive and Negative Syndrome Scale
Introduction
Attentional problems are one of the main cognitive deficits present in people diagnosed with schizophrenia Nuechterlein & Dawson [1]; Barch [2]; Goldberg & Bougakov [3]. One of the most widely-used tasks to assess attentional performance is the Continuous Performance Test (CPT). It consists of a task in which the individual must pay attention to the presentation of a series of stimuli on a computer screen and respond, generally by pressing a key, only when a fixed stimulus appears. From the development of the first CPT Rosvold et al. [4] there have been numerous versions; indeed, Greenberg & Waldman [5] suggested that there are more than 100 different types of CPT. There are endless differences between the tests (inter-stimulus interval, stimulus duration, frequency of target, total duration of the task, degraded stimulus, etc.), although all the tasks are considered to assess sustained attention. Most studies which assess attention using the CPT agree on the existence of a lower level of performance in people with schizophrenia, compared with healthy individuals Nuechterlein et al. [6]; Heinrichs & Zakzanis [7]; Riccio et al. [8]. In fact, this lower performance is not limited to acute episodes of the illness, but it continues once the symptoms have remitted Liu et al. [9]. These results have also been found in first-degree relatives of patients and in non-clinical individuals with schizotypal personality traits Keefe et al. [10]; Snitz et al. [11]. These findings have led to consider this deficit as a phenotypic marker of vulnerability to schizophrenia Cornblatt & Keilp [12]; Nuechterlein et al. [13], Pukrop et al. [14]. In general, the studies agree that as the difficulty of the CPT used increases, and therefore increasing the resources needed by the participants, the performance of patients with schizophrenia worsens, further distancing them from that of healthy control participants Vázquez et al. [15]. There are many studies which compare the CPT performance of people with schizophrenia with other samples, generally healthy control participants, but we have not found studies which compare the performance of different CPTs in the same sample; this would allow us to analyze the performance differences associated with each CPT, and therefore to understand specifically how the patients’ performance worsens according to the CPT used.
This is especially interesting considering the results obtained in the study by Ballard [16]. This author found different patterns in the performance of healthy control participants when comparing Conners’ CPT-no X with a CPT-AX, proposing that the two tasks could measure different cognitive skills. These differences in several parameters of the two CPTs could justify a difference between them beyond the difficulty of the task, involving in each case different cognitive process.
This study has used two tasks: a CPT-no X and a CPT-IP. In the CPT-no X the target is to press a key in response to all the stimuli which appear on the computer screen except one predetermined stimulus. In the CPT-IP the participant should respond only when the stimulus on the screen is identical to the previous stimulus. This means that there is a series of differences between the two tasks: in the CPT-no X the participant has to inhibit a repetitive motor response when the critical sign appears, whereas in the CPT-IP the participant has to make a response. In terms of the type of error committed, the CPT-no X would show up the inability to maintain a continued response over time (omissions) or to inhibit the response at a given moment (false alarms). In contrast, in the CPT-IP all the errors would reflect the inability to discriminate between stimuli.
The aim of the study is to compare the performance of these two types of task in a sample of patients with schizophrenia, and to analyze whether there is a relationship between the attentional performance in CPTs and the psychotic symptoms and socio-demographic characteristics of the sample.
Methods
Participants
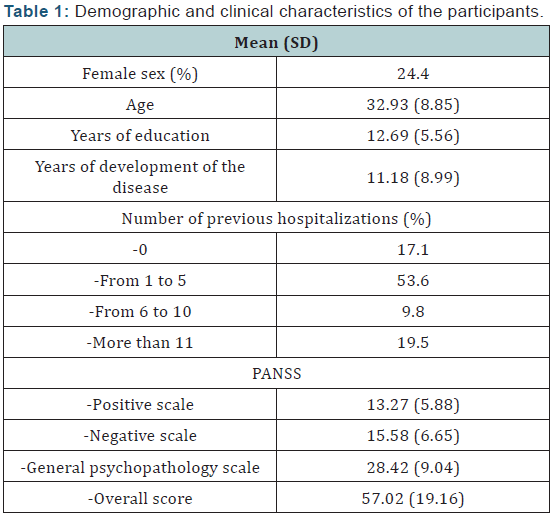
The sample consisted of 45 patients diagnosed with schizophrenia, 34 men and 11 women, with an average age of 32.93 (SD= 8.85) the characteristics of the sample are shown in (Table 1). All the participants were receiving medical treatment with antipsychotic drugs.
In order to take part in the study, the patients had to meet the following criteria: schizophrenia diagnosis according to DSM-IV APA [17]; stable symptoms during the previous month; and no cerebral damage, abuse/dependence on drugs, or diagnosis of other psychiatric conditions.
Measures
Conner’s Continuous Performance Test for Windows CPT II; Conners’ [18]. This CPT-no X consists of responding to all the letters which are shown on the computer screen except the letter ‘X’. The test is made up of 6 blocks of 60 trials each, and the total duration is 14 minutes. The frequency of appearance of the objective stimulus is 90%. In the analysis of the data, d’ as sensitivity index, the natural logarithm (Ln) of β as the indicator of the participants’ response bias, the hit rate (HR), the rate of false alarms (FAR) and the hits reaction times (RT) were used.
Continuous Performance Test -Identical Pairs (CPT-IP); Nuechterlein & Green [19]. In this CPT-IP the participants have to press a key each time they detect that the number shown on the screen is the same as the preceding number; that is, each time the same number appears consecutively. The task is divided into three parts: in the first the numbers have two digits, in the second three digits and in the third part four digits, leading to increasing difficulty. Each of the parts contains 120 trials. The total duration of the test is approximately 8 minutes. In the analysis of the data the indices d’, Ln β, HR, FAR and RT were used for each part of the test.
The Positive and Negative Syndrome Scale (PANSS); Kay et al. [20] Spanish adaptation of Peralta & Cuesta [21]. This scale is made up of 30 items which are scored on a scale of 1 to 7, during a semi-structured interview of 30-45 minutes in length. The items are grouped around three factors:
- Positive scale
- Negative scale
- General psychopathology scale.
For data analysis, the score for each scale was used along with the overall score of the test.
Procedure
Patients from the mental health centre who meet the requirements mentioned above were selected to take part in the study. In a first contact the over all aim of the study and the procedure to be followed during the assessment process were explained to them. If they agreed to take part, they signed the informed consent form, their clinical and demographic data were taken, and they did one of the two CPTs. In the following session they performed the other CPT (the order of the CPTs was counterbalanced) and the interview for the PANSS. In order to do the CPT, a laptop computer with a 17 inch screen was used. The participants used a standard mouse which allowed them to make their responses with their dominant hand.
Data analysis
For the analysis of the data the statistical analysis program SSPS v. 15.0 was used. The strategy used for the comparison of the performance between the two types of CPT was the Student t test (exploratory analysis showed the normal distribution of the data). A correlation analysis was carried out to analyze the relationship between attentional performance and psychopathology and socio demographic variables.
Results
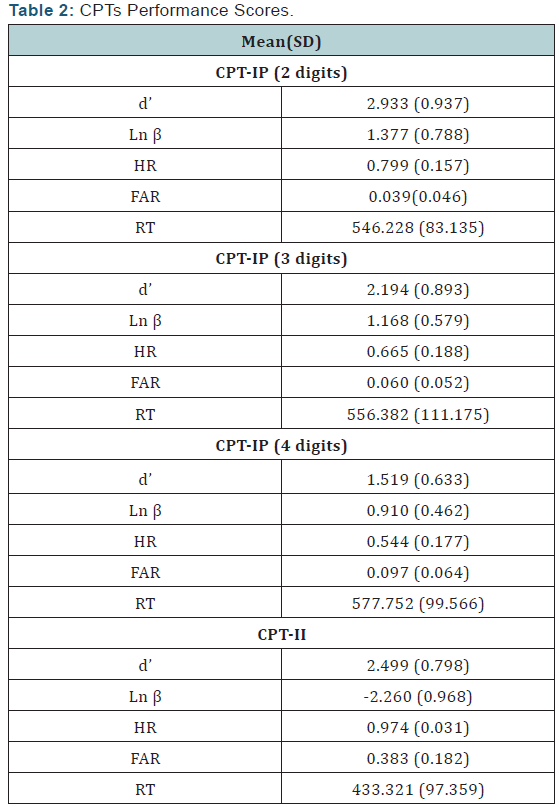
Means and standard deviation of cognitive measures tested are shown in (Table 2).
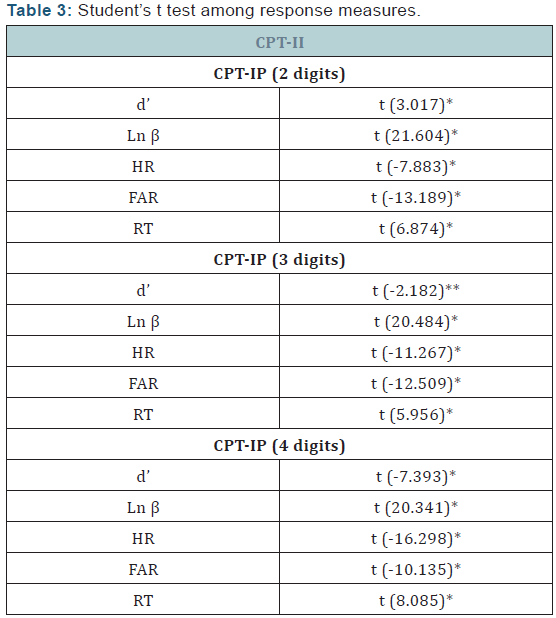
In order to compare the performance of the CPTs the indices d’, LN β, HR, FAR and RT were analyzed using the Student t test between each of the parts of the CPT-IP and the CPT-II1 (In a prior analysis of mean differences of the d’ of the three parts of the CPT-IP, we found significant differences between each part. Therefore, we decided to analyze each part independently). Significant differences were found in all the comparisons (Table 3).
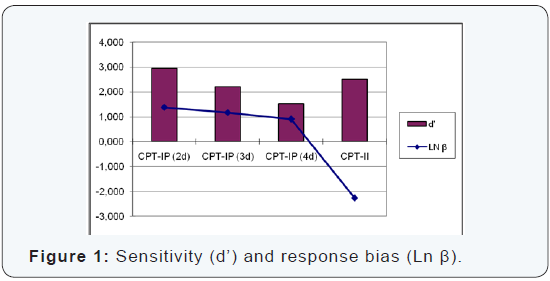
As (Table 2) shows, the sensitivity of the CPT-II is higher than that of the CPT-IP (expect for 2-digit), and the Ln β in the CPT-II is lower than that in the three parts of the CPT-IP. These differences can be seen clearly in the graphic shown in (Figure 1).
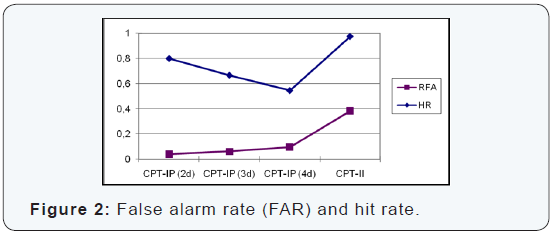
In terms of the change of criteria between both CPT, we can observe that the HR of CPT-II is higher than that of the three parts of the CPT-IP; the same applies to the FAR, as shown in (Figure 2).
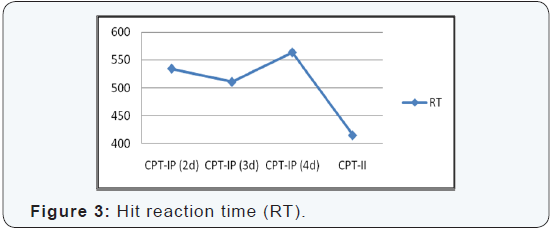
Finally, the RT is also different; in the CPT-II they are lower than those of the three parts of the CPT-IP (Figure 3).
The relationship between performance in the CPT and the other variables was analyzed using Pearson’s correlation coefficient. We found a significant relationship between educational level and the 3-digit CPT-IP (r=0.317; p<0.05) and the 4-digit CPT-IP (r=604; p<0.01).
Discussion
The aim of this study was to analyze the differences in the performance of patients with schizophrenia in the CPT-IP and the CPT-II. The results indicated that there are significant differences between all the variables studied. The first difference found in the analyses was different sensitivity (d’). Here, we found differences both between the three parts of the CPT-IP and between each of them and the CPT-II (the participants showed a level of sensitivity in the CPT-II which was lower than that of the 2-digit part of the CPT-IP and higher than that of the 3- and 4-digit parts).
This could be an effect of the differences in the difficulty of the task. Thus the CPT-IP, which is considered to be a highly demanding CPT and therefore more difficult, would generate (except in the most simple 2-digit part) lower performances than those seen in the CPT-II. This effect was found in the study by Vázquez et al. [22] in which a group of patients with schizophrenia and two groups with high and low schizotopy scores were compared in a CPT-DS and a CPT-X. The differences between the groups were seen only in the task with a high cognitive demand (CPT-DS); in addition, the worsening in performance from the simple task (CPT-X) to the difficult tasks (CPT-DS) was especially notable in the group of patients.
The response bias (Ln β) was also compared, and we found different response bias between both CPTs. Whereas in the CPTIP the participants’ criterion tended towards a conservative approach, in the CPT-II the participants became more liberal and took more risks, tending to give a response. These differences could be due to the frequency with which the target appears. In this sense, Silverstein et al. [23] manipulated the frequency of the target (30% and 75%) and found that the participants adopted a more liberal criterion at the same time as to increase the frequency.
In order to examine the participants’ response pattern, we analyzed the hit rates and the rates of false alarms. We found that response change led to a notable increase in both indices in the CPT-II; the participants increased their hit rate, but also the rate of false alarms. Therefore, it seems that it is not that one CPT is just easier than the other, but that they show different cognitive processes. These results are in line with those of Ballard [16] with healthy control participants, where the response patterns differed significantly when comparing the performance in Conners’ CPT with that of two standard CPT-AXs. Ballard did not use d’ nor Ln β, so it is not known how these indices would be affected; however, as in the present study, it was Conners’ CPT that had the highest commission error rates.
The differences in the different parameters of both CPTs suggest that there are different underlying processes at work. These differences between the two CPTs are not limited to performance patterns, and the RTs are also affected; whereas in the three parts of the CPT-IP the response speed was similar, in the CPT-II the RTs were greatly reduced. This could also be due to the different demands of each task. The fact the CPTIP demands a high level of resources involves a much more controlled and conscious processing, which would also imply more time Shiffrin & Schneider [24]. However, the CPT-II does not require participants to identify a complex sequence, but to recognize the letter X, which means fewer resources and less time are needed and leads to a faster response time Vázquez et al. [22]. In addition, higher target frequency is usually associated with lower RT Silverstein et al. [23], which may explain the differences in this parameter.
Summary
In summary, the differences observed in all the parameters analyzed seem to indicate that in patients with schizophrenia the two CPTs seem to respond to different underlying processes. The different target and cognitive load may be the principal variables which are responsible for these differences. The relatively high target frequency in the CPT-II and the relatively low resource demand together with faster TRs seem to reflect the presence of a more automatic response process, typical in relatively simple and monotonous tasks (only 10% of the trials involve a change of criteria). The more lax response bias might reflect the difficulty of these processes in adapting to the change of the task with the appearance of the letter X. It could be hypothesized that the CPT-II shows to a greater degree the use of an executive control on these more automatic processes, similar to that found in dual tasks in which the automation process is made more difficult because the complexity of the task Granholm et al. [25]. Furthermore, the CPT-IP implies more controlled processing, in which each stimulus has to be compared to the previous one, which leads to a much more complex task (especially if the number of digits is increased); this makes the use of automatic processes more unlikely. This would be reflected in higher RTs and in a much stricter response bias (although performance is worse).
Conclusion
The results found highlight the importance of using different measures of participants’ performance in CPT tasks, since taking into account only sensitivity (d’) can lead to the omitting of relevant information which is necessary for a right interpretation. It would be useful to carry out a study in which each CPT was applied repeatedly, in order to find out whether with repetition of the task, the participants’ performance depended to a greater degree on more automatic processes, in which case there would be little improvement in performance, or on more controlled processes, in which case performance would benefit greatly from practice Neisser [26].
Another relevant result found in the present study is the significant relationship between the 3- and 4-digit parts of the CPT-IP and number of years in education of the participants. These tasks seem to depend to a greater extent on controlled processes, especially the 4-digit part which is where the strongest correlation was found. In a study by Gonzalez-Andrade [27], a significant correlation was found between the number of years in education and an indicator of divided attention obtained in the performance of dual tasks. This suggests that these CPT tasks, which are less automated, would be more influenced by educational and learning components.
Acknowledgment
This research has been financed by the Health Department of The Andalusian Government (PI-0152/2008).
References
- Nuechterlein KH, Dawson ME (1984) Information processing and attentional functioning in the developmental course of schizophrenic disorders. Schizophrenia Bulletin 10(2): 160-202.
- Barch DM (2005) The cognitive neuroscience of schizophrenia. Annual Review of Clinical Psychology 1: 321-353.
- Goldberg E, Bougakov D (2005) Neuropsychologic assessment of frontal lobe dysfunction. The Psychiatric Clinics of North America 28(3): 567-580.
- Rosvold HE, Mirsky A, Sarason I, Bransome ED, Beck LH (1956) A Continuous Performance Test of brain damage. Journal of Consulting Psychology 20(5): 343-350.
- Greenberg LM, Waldman ID (1993) Developmental normative data on the Test of Variables of Attention (TOVA). Journal of Child Psychology and Psychiatry 34(6): 1019-1030.
- Nuechterlein KH, Dawson ME, Ventura J, Fogelson D, Gitlin M, et al. (1991) Testing vulnerability indicators across clinical state. En: Häfner Hy, Gatta WF (Eds.), Search for the causes of schizophrenia, Springer- Verlag, Berlin,Germany, pp. 177-191.
- Heinrichs RW, Zakzanis KK (1998) Neurocognitive deficits in schizophrenia: a quantitative review of the evidence. Neuropsychology 12(3): 426-445.
- Riccio CA, Reynolds CR, Lowe PA (2001) Clinical applications of Continuous Performance Test. John Wiley & Sons, Canada.
- Liu SK, Hsieh MH, Hwang TJ, Hwu HG, Liao SC, et al. (2006) Reexamining sustained attention deficits as vulnerability indicators for schizophrenia: stability in the long term course. Journal of Psychiatric Research 40(7): 613-621.
- Keefe RS, Perkins DO, Gu H, Zipursky RB, Christensen BK, et al. (2006) A longitudinal study of neurocognitive function in individuals at-risk for psychosis. Schizophrenia Research 88(1-3): 26-35.
- Snitz BE, Macdonald AW, Carter CS (2006) Cognitive deficits in unaffected first-degree relatives of schizophrenia patients: a metaanalytic review of putative endophenotypes. Schizophrenia Bulletin 32(1): 179-194.
- Cornblatt BA, Keilp JG (1994) Imparied attention, genetics, and pathophysiology of schizophrenia. Schizophrenia Bulletin 20(1): 31- 46.
- Nuechterlein KH, Dawson ME, Green MF (1994) Informationprocessing abnormalities as neuropsychological vulnerability indicators for schizophrenia. Acta Psychiatrica Scandinavica. 384: 71- 79.
- Pukrop R, Ruhrmann S, Schultze-Lutter F, Bechdolf A, Brockhaus- Dumke A (2007) Neurocognitive indicators for a conversion to psychosis: comparison of patients in a potentially initial prodromal state who did or did not convert to a psychosis. Schizophrenia Research 92(1-3): 119-125.
- Vázquez C, Nieto-Moreno M, Cerviño MJ, Fuentenebro F (2006) Efectos del incremento de la demanda cognitiva en tareas de atención sostenida en los trastornos esquizofrénicos y la esquizotipia. Psicothema 18(2): 221-227.
- Ballard JC (2001) Assessing attention: comparison of responseinhibition and traditional Continuous Performance Test. Journal of Clinical and Experimental Neuropsychology 23: 331-350.
- American Psychiatric Association (1994) Diagnostic and Statistical Manual of Mental Disorders, (4th edn). APA Press, Washington D.C, USA.
- Conners CK (2004) Conners’ Continuous Performance Test for Windows (CPT II). Multi-Health System Inc, Canada.
- Nuechterlein KH, Green MF (2006) MATRICS Consensus Cognitive Battery. MATRICS Assesment, California, USA.
- Kay SR, Fiszbein A, Opler LA (1987) The positive and negative syndrome scale (PANSS) for schizophrenia. Schizophrenia Bulletin 13(2): 261-276.
- Peralta V, Cuesta ML (1994) Validación de la escala de los síndromes positivo y negativo (PANNS) en una muestra de esquizofrénicos españoles. Actas Luso-Españolas de Neurología, Psiquiatría y Ciencias Afines 22: 171-177.
- Vázquez C, López B, Florit A (1996) Procesamiento de la información y esquizofrenia: hallazgos empíricos y bases teóricas para la rehabilitación. En: Aldaz LA, Vázquez C (comps.), Esquizofrenia: fundamentos psicológicos y psiquiátricos de la rehabilitación. Siglo XXI, Madrid, pp. 23-55.
- Silverstein ML, Weinstein M, Turnbull A (2004) Nonpatient CPT performance varying target frequency and interstimulus interval on five response measures. Archives of Clinical Neuropsychology 19(8): 1017-1025.
- Shiffrin RM, Schneider W (1977) Controlled and automatic human information processing: Detection, search, and attention. Psychological Review 84: 1-66.
- Granholm E, Marder SR, Asarnow RF (1996) Dual-task performance operanting characteristics, resource limitations, and automatic processing in schizophrenia. Neuropsychology 10(1): 11-21.
- Neisser U (1976) Psicología cognoscitiva. Trillas, México, USA.
- González-Andrade A (2008) Estudio de la atención dividida mediante un paradigma de tareas duales en una muestra de pacientes con esquizofrenia. Non published doctoral dissertation. University of Jaén, Europe.
