




Executive Dysfunction in Depression
*Lt Col Shahabaz Ali Khan, Shagufta Khanam, Ryali VSSR, Srivastava K, Bhat PS and Prakash J
Guru Gobind Singh Indraprastha University, India
Submission: April 21, 2016; Published: May 09, 2016
*Corresponding author: Shahbaz khan, Delhi Cantonment, Guru Gobind Singh Indraprastha University, Tel: 08002404433; Email:shahbaaz323@yahoo.com
How to cite this article: Lt Col Shahabaz A K, Shagufta K, Ryali VSSR, Srivastava K, Bhat PS, et al. Executive Dysfunction in Depression. Psychol Behav Sci Int J. 2016; 1(2) : 555556. DOI: 10.19080/PBSIJ.2016.01.555556
Introduction
Executive dysfunction is common in Major depression and includes problems with planning, organizing, sequencing, shifting, information processing speed, and maintaining information in working memory [1,2]. The relationship is complex and adds to the disability [3]. The test commonly used for executive function in psychiatric disorders is the Wisconsin Card Sorting Test (WCST) [4]. Studies have shown that WCST scores may be affected even with relatively mild depression [5] and executive dysfunction may vary as a function of the severity of depression [6]. However, some studies found no such relationship between severity of depression and the overall cognitive performance [7]. Moreover, only a few studied executive dysfunctions in young depressives [8]. In the present study we compared the executive functions in depression with healthy controls and attempted to see whether there is any difference in executive function in depressives and non depressed matched healthy controls. Also we wanted to see whether the first time depressed differ from the depressed who have recurrent depression. The effect of severity of depression on the executive functions was also assessed.
Abbreviations
BDI: Beck’s Depression Inventory; WCST: Wisconsin Card Sorting Test; GHQ: General Health Questionnaire; ANOVA: Analysis of variance; ME: Multiple Episode Depressives; FE: First Episode Depressives
Method
This cross sectional analytical controlled study included cases of major depression with or without history of past depression, diagnosed as per ICD 10 DCR (F32) and F (33) using structured interview DSM IV, between ages of 21 to 50 years presenting to psychiatry OPD. Co-morbid psychiatric illness, bipolar disorder, hypo/hyperthyroidism, head injury, substance abuse were excluded. Local ethical committee gave clearance. Beck’s Depression Inventory (BDI) was administered to quantify the depression severity into mild, moderate or severe. Wisconsin Card Sorting Test (WCST) (64 card, computerized version) was administered to all patients for the assessment of executive functions. For comparison, 50 healthy subjects matched with respect to age, gender, handedness, and educational level were selected. Controls were also screened for family history of depression. They were administered the General Health Questionnaire (GHQ – 60, with an inclusion score of <12) to rule out any significant psychiatric morbidity.
Analysis of Data
Using SPSS18, normally distributed continuous variables were analyzed with independent t-tests. Analysis of variance (ANOVA) was used for multiple comparisons.
Results
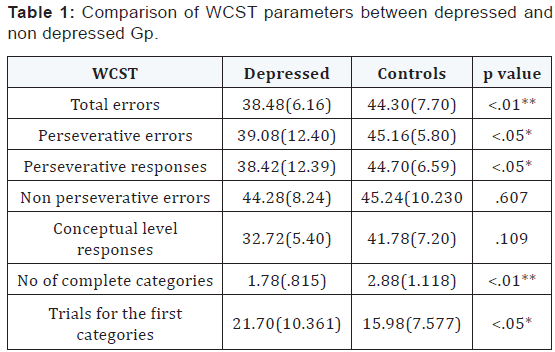
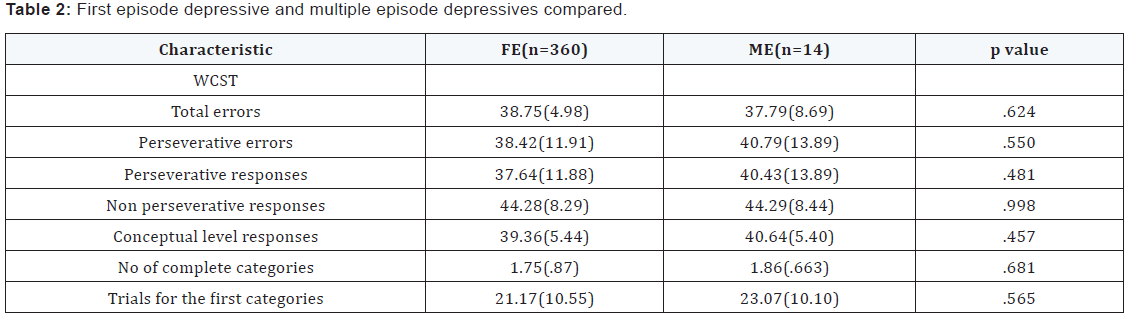
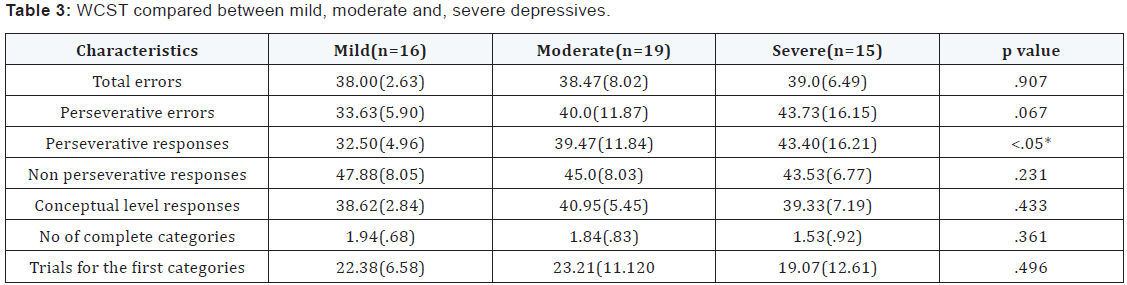
Patients with major depression and healthy controls did not differ significantly in age, marital status, education or handedness. All patients and control subjects were males. In the recurrent depressive group the average no of past episodes of depression was 2.305 with a history of ECTs in 3 patients. There was a significant difference between the depressed group and the non depressed healthy controls on various measures of WCST measured executive functions - Total errors, perseverative errors, perseverative responses, no of complete categories and trials for the first category domains. Noteworthy was the finding that the FE depressives and the ME depressives did not differ on any WCST parameters significantly. There was a significant difference between the mild, moderate and severe depressives in terms of perseverative responses. No other difference was noted (Table 1-3).
Discussion
The main findings of this study were:
- As a group when compared to the non depressed healthy controls, the depressed patients performed poorly on several measures of executive functions.
- Currently depressed patients who had a past burden of depressive illness (ME) were no different from the First Episode depressives in terms of Executive dysfunction.
- When seen across the ICD 10 severity specifiers (mild, moderate, severe), significant difference was seen only in perseverative responses.
The presence of executive dysfunction in depression as brought out in this study is in conformity with previous such studies worldwide underlining the fact that cognitive deficits esp. executive dysfunction is also a core feature of depression [6]. It is interesting to surmise whether these neurocognitive deficits in depression can help us localize the neuropathology in depression which eludes us till date. The link between executive function and emotion is worth exploring. The WCST typically involves working memory and context dependent memory where the previous context has to be kept in mind and used as a template to make current shifts in attention, using positive and negative feedbacks on the answers given. In this context recent research has focused on hippocampus and its connection [9]. The domains assessed by the WCST seems to be subserved by a fronto-subcortical circuit that originates in the dorsolateral prefrontal cortex and orbitofrontal cortex and then projects through the striatum and thalamus to return to the prefrontal cortex. However, the hippocampus may also influence these networks as concluded by Wall and Messier [10] that the hippocampus–oribitomedial prefrontal circuit can efficiently contribute to the integration of cognition, emotion and behavior and can thus influence working memory and executive functions. In line with this hypothesis a recent fMRI study brought out the fact that depressed patients, as compared to normal controls had decreased activation of hippocampus on cognitive function tasks and different hippocampal region showed variable hypo activation [11]. This apparent localization to quite a small brain area of a critical link between affect and cognition comes as something of a surprise, but it is supported by a number of functional imaging studies and by some recent neuropsychological studies in depression [12]. It would be interesting to see whether these cognitive deficits persist after remission of depression i.e whether they are state dependent or trait. Unfortunately, the present study design did not permit us to comment on whether there are persistent executive function deficit in depression for which a before and after follow up study is required. The fact that executive functions are not significantly different between the mild, moderate and severe depressives (except preservative responses), underlines the hypotheses that the DSM IV differentiation with respect to severity may be only a phenomenological observational differentiation not based on neuro/psychobiology. It may be so that perseveration may be a more fundamental neuropsychological domain and better correlating with the severity of depression [13].
Conclusion
The fact that the various factors of WCST dysfunction are not a function of depression severity also proves that the deficits seen in depression are not a direct result of general demotivation and negative approach towards the test itself, or else the deficits seen would show gradient with increasing severity of depression i.e the more demotivated (moderate and severe depressed) would show increasing deficits in executive on WCST as compared to mild. As far as the burden of previous depressive illness is concerned, this study confirms that Multiple Episode depressives (ME) and first Episode depressives (FE) are similar when assessed for the performance on various WCST parameters and cumulative illness did not affect their performance. But to conclude that cumulative illness has no effect on executive functions without doing a “before and after” serial WCST measurement study would be premature.
References
- Fossati P, Ergis AM, Allilaire JF (2002) Executive functioning in unipolar depression: a review. Encephale 28(2): 97-107.
- Stordal KI, Lundervold AJ, Egeland J, Mykletun A, Asbjornsen A, et al. (2004) Impairment across executive functions in recurrent major depression. Nord J Psychiatry 58(1): 41-47.
- Harvey PO, Le Bastard G, Pochon JB, Levy R, Allilaire JF, et al. (2004) Executive functions and updating of the contents of working memory in unipolar depression. J Psychiatr Res 38(6): 567-576.
- Heaton RK, Chelune GJ, Talley JL, Kay GG, Curtiss G (1993) Wisconsin Card Sorting Test Manual: Revised and expanded. Psychological Assessment Resources. Odessa, Florida.
- Feil D, Razani J, Boone K, Lesser I (2003) Apathy and cognitive performance in older adults with depression. Int J Geriatr Psychiatry 18(6): 479-485.
- Totic-Poznanovic S, Marinkovic D, Tomic G, Paunovic VR (2006) Executive functions in young patients with unipolar depression. Srp Arh Celok Lek 134(7-8): 273-277.
- Merriam EP, Thase ME, Haas GL, Keshavan MS, Sweeney JA (1999) Prefrontal cortical dysfunction in depression determined by Wisconsin Card Sorting test performance. Am J Psychiatry 156(5): 780-782.
- Purcell R, Maruff P, Kyrios M, Pantelis C (1997) Neuropsychological function in young patients with unipolar major depression. Psychol Med 27(6): 1277-1285.
- Totić-Poznanović S, Marinković D, Tomić G, Paunović VR (2006) Executive functions in young patients with unipolar depression. Srp Arh Celok Lek 134(7-8): 273-277.
- Frodl T, Meisenzahl EM, Zetzche T, Born C, Groll C, et al. (2002) Hippocampal changes in patients with a first episode of major depression. Am J Psychiatry 159(7): 1112-1118.
- Wall PM, Messier C (2001) The hippocampal formation-orbitomedial prefrontal cortex circuit in the attentional control of active memory. Behav Brain Res 127(1-2): 99-117.
- Videbech P, Ravnkilde B (2004) Hippocampal volume and depression: a meta-analysis of MRI studies. Am J Psychiatry 161(11): 1957-1966.
- Murphy FC, Sahakian BJ, Rubinsztein JS, Michael A, Rogers RD, et al. (1999) Emotional bias and inhibitory control processes in mania and depression. Psychol Med 29(6): 1307-1321.
