



Guidelines. A Word of Caution.
Z Giovanni D Tebala*
Division of Surgery, Noble’s Hospital, Isle of Man
Submission: July 20, 2016 ; Published: July 21, 2016
*Corresponding author: Giovanni D Tebala, Division of Surgery, Noble’s Hospital Strang, Douglas, Isle of Man, IM4 4RJ, Tel:+441624650000; Email: Giovanni.Tebala@gov.im
How to cite this article: Giovanni D T. Guidelines. A Word of Caution. Open Access J Surg. 2016; 1(2): 555558.DOI: 10.19080/OAJS.2016.01.555558
Editorial
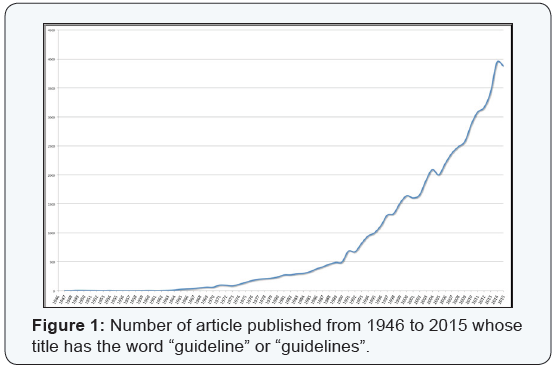
A good healthcare system should produce evidences, not guidelines. Evidences should then be judged and evaluated case-by-case and the single professional should be able to decide what is the best treatment for that single patient on the basis of good evidences, not following someone else’s judgment that can be biased by many external and non-clinical factors. The number of published guidelines has exponentially increased in the last 70 years (Figure 1) and, according to one of the most used medical Literature database we queried with “(guideline[Title]) OR guidelines[Title]”, 2691 articles reporting the word “guideline” or “guidelines” have been published in the first six months of 2016. It must be specified, however, that not all these articles actually report clinical guidelines and some of them are critical appraisals of previously published guidelines.
Guidelines have been defined as “systematically developed statements to assist practitioner and patient decisions about appropriate health care for specific clinical circumstances” [1]. Who decides this is appropriate? Usually, a committee of “experts” surfs within the available Literature and select the best evidences to construct guidelines on. They meet one or more times and write down statements to be passively followed by all kind of healthcare practitioners. The so-called “relevant” Literature can be unbalanced by publication bias and the selection process can be biased by the expert’s personal experience, angle-of-view of the problem, personal interests, and other external confounding factors [2]. Then they produce statements that, in the best case, are rigid and general and may not lead to the best decision for the specific patient. Last, but not least, Literature evidences are usually many months - if not years - ahead of guidelines, due to the length of the process leading from publication of evidences to publication of guidelines (Literature selection, committee meetings, text drafting, editing, and publishing). One may argue that guidelines are generic and are only meant to “guide” the clinician’s decision. Unfortunately, this is not true, as nowadays guidelines are used as a sort of sacred book containing the universal and unchangeable truth. They cannot be challenged, only passively followed.
Once upon a time there was a mad bandit who lived in a forest. His name was Procrustes. He had the strange habit of abducting anyone who risked his way into the forest and tying him/her on his bed, the famous Procrustes’ bed. Those that were too short for the bed were stretched to fit and those who were too tall had their excess length amputated. Obviously, no one survived. Are we treating our patients with a Procrustean method? Stretching them to fit our rigid guidelines? Are we abdicating our role of cultural leaders? Is medical community so ignorant to need someone to teach them how to think and how to consider evidences? Is this a proof of failure of the University system? Guidelines are crucial in systems where those who actually deliver the service are not skilled and theoretically able to take critical decisions, so someone else decided on their behalf beforehand. What are we teaching our medical students?
What is the point of spending hours on Pharmacology books if the treatment of pneumonia has been already decided and standardized by some expert committee? They don’t need to decide, don’t need to evaluate; ultimately they don’t need to think. I am afraid that the rise of the number of guidelines - there are guidelines for everything - may be demonstrated to be inversely related to the knowledge and skills of doctors, nurses, practitioners. Is it a case that we live and work within a healthcare global system where non-medically-graduated professionals are taking over? Another may correctly argue that guidelines are useful to standardize our care. Are we sure that standardizing is in the best interest of our patients? If we treat all our patients in the same way, how can we be sure this is the best way? Improvement is in diversity and evolution is when someone stands out from the average.
At a point in history a single fish, while happy in the sea, nevertheless decided he wanted to explore the dry land, despite “guidelines” suggested that fishes should stay safe in the water. One argument favoring clinical guidelines is that they can be useful to reduce expenditure in a system that is already under pressure [3]. Unfortunately, in this sentence there is a selfcontradiction. Clinical guidelines are clinical, not economical. They are supposed to support the best interest of the patient, not the financial accounts of the trust. As economics play a central role in healthcare, clinical guidelines should - at a second time - be benchmarked against the available resources, but this is a further step beyond the clinical decisions, otherwise we run the risk - very actual indeed - to transform clinical medicine into finance based medicine [2]. Guidelines are the misunderstood consequence of evidence-based medicine (EBM). EBM has been defined as “integrating individual clinical expertise with the best available external clinical evidence from systematic research” [4].
This definition of EBM leaves to the single professional the commitment - and the intellectual pleasure – to evaluate evidences and integrate them with his or her own experience and expertise to deliver the best healthcare. Unfortunately, this is not reflected in everyday practice, where guidelines are the “despots” that rule our job with no space at all for personal and individual experience, knowledge and skills. A machine or a monkey could do our work in the future if we don’t put back official guidelines to their correct position and cultural role of clinical and cultural suggestions and advices. This role is crucial in the development of medicine and in stimulating discussions and brain storming. Let’s leave our minds and hearts and hands doing our job and dealing with our patients.
References
- Field MJ, Lohr KN (1990) Clinical Practice Guidelines: Directions for a New Program. Institute of Medicine (US) Committee to Advise the Public Health Service on Clinical Practice Guidelines, Washington (DC): National Academies Press (US).
- Ioannidis JP (2016) Evidence-based medicine has been hijacked: a report to David Sackett. J Clin Epidemiol 73: 82-86.
- Langell JT, Bledsoe A, Vijaikumar S, Anderson T, Zawalski I, et al. (2016) Implementation of national practice guidelines to reduce waste and optimize patient value. J Surg Res 203(2): 287-292.
- Sackett DL, Rosenberg WMC, Gray JAM, Haynes RB, Richardson WS (1996) Evidence based medicine: what it is and what it isn’t. BMJ 312(7023): 71-72.
