




Metastatic Lung Adenocarcinoma Mimicking an En-Plaque Meningioma: Case Report
Jasmit Singh M Ch1*, Florian Ebner2 and MarcosTatagiba3
Department of Neurosurgery, Eberhard-Karls-University of Tubingen, Germany
Submission: October 27, 2017; Published: December 14, 2017
*Corresponding author: Jasmit Singh M Ch, WFNS Fellow, Department of Neurosurgery, Eberhard-Karls-University of Tubingen, Tubingen, Germany, Tel: +917087428294; Email: jasmeetthukral80@gmail.com
How to cite this article: Jasmit S M C, Florian E, Marcos T . Metastatic Lung Adenocarcinoma Mimicking an En-Plaque Meningioma: Case Report. Open Access J Neurol Neurosurg. 2017; 6(4): 555692. DOI: 10.19080/OAJNN.2017.06.555692
Abstract
Dural based lesions in the cranium may result secondary to benign or malignant pathology that may be sometimes difficult to differentiate on imaging. Detailed clinical evaluation and high index of suspicion in many cases will narrow the differential diagnosis. We report an extremely rare case of lung adeno-carcinoma metastasis to brain which appeared as an En-plaque meningioma on neuro-imaging. A benign-appearing dural- based en-plaque lesion may be a manifestation of an underlying malignancy, and a thorough clinical and radiological examination is mandatory to avoid misdiagnosis.
Background
Cerebral metastases are the most frequent brain tumors in adults and they may rarely present as an isolated meningeal mass, suggesting a meningioma [1]. The radiographic features do not necessarily differentiate between meningioma and metastatic dural-based tumors [1]. We report a very rare case of an elderly patient who presented with en-plaque dural based lesion resembling a meningioma. Histopathology was consistent with metastatic adenocarcinoma. This case highlights the importance of also considering metastasis during the work-up of an elderly patient with a new dural-based lesion that mimics meningioma (based on radiographic studies), and should prompt additional body imaging to search for the primary.
Case Summary
An 80-year-old right handed female presented to us with a 2 month history of hemicranial headache localized to right side. Headache was worse in morning and had progressed in severity over 2 months. There were no constitutional symptoms. Neurological examination did not reveal any neurological deficit. She had history of hysterectomy (for fibroid uterus) and dental surgery in the past; she was also a known case of hypertension and diabetes mellitus. In particular, there was no recent history of weight loss and no abdominal or genitourinary symptoms.
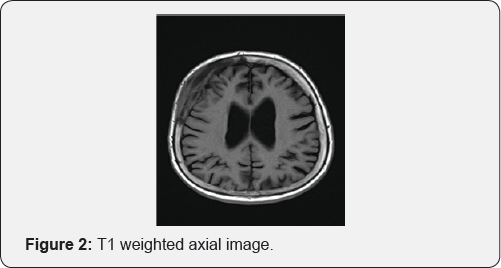
MRI brain revealed an en-plaque contrast enhancing lesion involving the dura of right fronto-temporal region, with changes in overlying bone (Figure 1). The lesion was iso-intense on T1 weighted images (Figure 2) and hyperintense on T2 weighted image (Figure 3); radiologically resembling an en-plaque meningioma. Though the presumed radiological diagnosis was strongly in favor of meningioma; considering her age, differential diagnosis of en-plaque meningioma Vs metastasis Vs a primary calvarial lesion was made. Metastatic work up included CT scan of abdomen and chest was performed. Chest CT showed suspicious lesion in right upper lobe which did not reveal any malignancy on percutaneous biopsy (repeated twice). Since patient was symptomatic she was given option of surgery. She underwent right fronto-temporal craniotomy under general anesthesia. The tumor was seen involving the dura as a thin sheath. There was an area of parenchymal involvement, but it could be resected without difficulty. The bone was involved in disease and was not replaced, cranioplasty was done using acrylic (Figure 4). The post-operative course was uneventful with the patient completely recovering with no neurological deficit (Figure 5). On intraoperative smear and frozen section, the diagnosis of metastatic adeno-carcinoma was rendered. It was confirmed with final histopathology and immuno- histochemistry of the tumor, which revealed features consistent with metastatic adenocarcinoma of likely lung origin.





Discussion
Direct dural involvement by an underlying intracerebral metastasis is not uncommon. However, true dural metastases are rare. Dural involvement in metastatic lesions may be due to direct extension of metastatic skull metastases or by hematogenous spread through venous or arterial dissemination from the primary site [2]. Of the dural-based metastatic lesions, carcinomas of breast, lung and prostate have been the most commonly reported [2]. Typically, these tumors produce MRI images with increased signals on T2-weighted images and often with an enhancing dural tail mimicking a meningioma [2]. However, radiological presentation of dural-based metastasis as purely en plaque variety is extremely rare and has been seldom reported in literature. Unlike En-plaque meningioma which exhibits characteristics on MRI sequences, dural based en-plaque metastasis may exhibit some atypical features like disproportionate edema, the highly irregular and nodular surface of the lesion, the presence of a heterogeneous interface between the lesion and the normal brain , and partial or complete disappearance of the peritumoral band [3].
The diagnostic dilemma between meningioma and dural metastases is of increasing importance because of changing paradigms in the management of both these tumors. Off late there has been an increasing tendency to manage asymptomatic meningioma conservatively with serial radiological imaging; and also there have been remarkable changes in the medical management of disseminated malignancies that has led to their non-surgical management. Surgical resection of meningioma is not without morbidity, with a significantly higher risk being identified in geriatric patients. A non-surgical approach of expectant observation with regular scans, reserving surgery for cases exhibiting significant tumor growth or becoming symptomatic is not uncommonly advocated for elderly or infirm patients. This will be devastating in case of metastatic disease where the life expectancy is limited due to aggressive tumor behavior. Similarly, radiosurgery without histological diagnosis is also sometimes advocated for presumed meningioma in the elderly, based primarily on the radiographic findings. New tools like MR spectroscopy of metastases have been found to have different lipid signals and lactate peaks [4]. But the accuracy is still to be determined in prospective studies and it may not be readily available at many centers. Therefore it is important to discuss the risk of misdiagnosis with the patients who are being treated with working diagnosis of meningioma without histological diagnosis. A repeat imaging is strongly recommended in these cases at-least 3 months or earlier if there is any unexpected change in clinical condition [4].
Our patient had an En-plaque dural lesion which was presumed to be a meningioma. But her age and short history raised the suspicion. Although her CT scan of chest revealed atypical lesion, biopsy was negative for malignancy. There was no associated mass effect from the lesion, and considering her age patient could have been followed with serial scans based on radiographic findings. But given her age, the local headaches and suspicious lesion in chest we discussed the chances of misdiagnosis with patient and gave her option of resection. It eventually turned out to be a metastatic adenocarcinoma. It is most important to analyze the imaging meticulously, keeping differentials rather than going ahead with a single diagnosis. The role of proper and detailed history cannot be over-emphasized in these cases. Elderly patient, constitutional symptoms, short duration of history, past history of malignancy, subtle atypical findings on radiology should always be viewed with suspicion [2,3]. It is prudent to have a detailed work-up for primary in these cases.
Conclusion
Although they are uncommon, dural metastases can be mistaken for meningioma. The importance of this entity amongst the clinicians cannot be over-emphasized. Metastasis should always feature in the list of differential, even for a relatively benign looking en plaque lesion especially with rapid clinical progression or in elderly patient.
References
- Tagle P, Villanueva P, Torrealba G, Huete I (2002) Intracranial metastasis or meningioma? An uncommon clinical diagnostic dilemma. Surg Neurol 58(3-4): 241-245.
- Ankur K, Amey S, Chaterjee D, Salunke P, Vasishta RK, et al. (2015) Dural metastasis masquerading as an en plaque meningioma. J Neurosci Rural Pract 6(3): 420-422.
- Satoshi T, Ikuo S, Koichi O, Jiro W, Toshio S, et al. (2004) Neuroradiological findings of atypical meningiomas. CMIG Extra: Cases 28: 33-39.
- Laidlaw JD, Kumar A, Chan A (2004) Dural metastases mimicking meningioma. Case report and review of the literature. Journal of Clinical Neuroscience September 11(7): 780-783.
















{kind=link}