



Can Magnetic Resonance Urethrography (MRU) be a Single-Stop Shop for Male Urethral Stricture Evaluation?
Sagar Parashar and Vijai Pratap
Department of Radio Diagnosis, Teerthanker Mahaveer Medical College and Research Center, Moradabad, Uttar pradesh, India
Submission: October 02, 2016; Published: October 21, 2016
*Corresponding author: Rajul Rastogi, Department of Radio Diagnosis, Teerthanker Mahaveer Medical College and Research Center, Moradabad, U.P, India.
How to cite this article: Rajul R, Pawan J, Yuktika G, Shourya S, Pankaj K D, et al. Can Magnetic Resonance Urethrography (MRU) be a Single-Stop for Male Urethral Stricture Evaluation?. JOJ uro & nephron. 2016; 1(1): 555555. DOI: 10.19080/JOJUN.2016.01.555555
Abstract
Stricture in male urethra is a commonly encountered clinical condition in urological outpatient department. Till recently, all such strictures were being evaluated with Retrograde Urethrography (RGU) to determine the future course of management. But with the advent of plastic surgery, information regarding presence of spongiofibrosis & other associated conditions, in addition to length of stricture is being demanded from radiologist for deciding the mode of management. Hence, this article discusses various imaging modalities for evaluation of male urethral strictures with their merits and demerits in the light of recent medical literature.
Keywords: Magnetic resonance; Retrograde; Urethrography; Urethral; Stricture; Spongiofibrosis Abbrevations: MUS: Male Urethral Strictures; PUS: Perirethral Spongiofibrosis; MCU: Micturating Cystourethrography; SUG: Sonourethrography; MRU: Magnetic Resonance Urethrography; VCUG: Video Cystourethrography
Introduction
Male urethral strictures (MUS) are broadly divided in to anterior and posterior urethral strictures depending upon location, each with different set of causes. Anterior urethra may show luminal narrowing / stricture leading to obstructive urinary symptoms usually secondary to extrinsic causes (straddle injury, catheterisation / iatrogenic instrumentation) and intrinsic causes (urethral infection / inflammation or balanitis xerotica obliterans) which may or may not be associated with fibrosis in corpora spongiosum adjacent to stricture site known as periurethral spongiofibrosis (PUS) [1]. Posterior urethral strictures are usually secondary to external injury with or without loss of urethral axis and subsequent fibrosis or scar formation [1]. Imaging evaluation of male urethral strictures can be done by retrograde urethrography (RGU) with micturating cystourethrography (MCU), sonourethrography (SUG) and magnetic resonance urethrography (MRU). This article discusses the merits and demerits of various imaging modalities in evaluation of MUS.
Discussion
Except for rare cases which resolve spontaneously [1], MUS require treatment which may range from simple dilatation & internal urethrotomy to stent placement & reconstructive procedures, the choice of which predominantly depends upon the site as well as length of stricture; presence & extent of PUS; presence of urethral destruction; loss of urethral axis and presence of other associated findings like presence of urethral calculus, sinus or fistula, diverticulum, etc. [2].
Simple dilatation and visual / endoscopic internal urethrotomy is useful in short segment (<1.5cm) urethral strictures without PUF while longer strictures (>1.5cm) & presence of PUF necessitate open reconstructive surgeries to reduce procedure-failure & recurrence rates [3]. Since long, retrograde urethrography (RGU) has remained the mainstay of evaluating MUS, determining mode of management until recently when sonourethrography (SUG) and magnetic resonance urethrography (MRU) emerged as revolutionising imaging techniques [4,5].
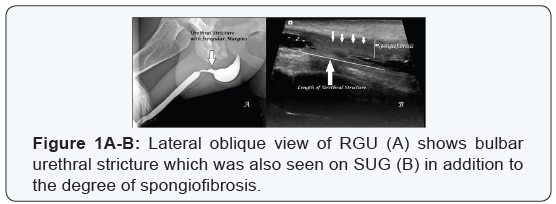
RGU is a simple, easily available & inexpensive method of evaluating location and length of anterior male urethral strictures in experienced hands with accuracy approaching to that of SUG & MRU (Figure 1A) [1]. However, the major limitations being technical expertise consisting of patient positioning, traction & positioning of penis and optimal injection pressure necessary for adequate distension of the urethral lumen [thus avoiding false diagnosis of urethral stricture as high injection pressure can produce forceful reflex contraction of pelvic musculature] as well as mucosal injury / sepsis and rarely anaphylactic shock secondary to intravasation of iodinated contrast medium especially in cases of acute traumatic urethral injuries [1,6].
In addition, the radiation risk to gonads cannot be undermined in those requiring repeated evaluation for residual or recurrent disease. Also the information provided is limited to luminal disease. RGU combined with video-cystourethrography (VCUG) often do not provide adequate information required for plastic reconstruction as delineation of posterior urethra is often suboptimal and there is no information regarding the presence & degree of PUF as well as prostatic-urethral axis displacement [7].
SUG became popular in evaluation of MUS in last decade of 20th century due to its inherent advantage of being radiation free and relatively non-invasive [1,8]. Recently, the role of sonoelastography has been suggested in evaluation of MUS further improving the significance of SUG [9]. Accuracy of SUG is comparable to RGU & MRU in anterior MUS with additional advantage of detecting the presence & extent of PUF (Figure 1B) [1,10]. However, though major limitations of SUG are operator dependence, small field of view and failure to achieve optimal information about posterior urethra & urethral diverticulum / fistulae yet it is superior to RGU in characterising intraluminal urethral lesions including urethral tumours [10].
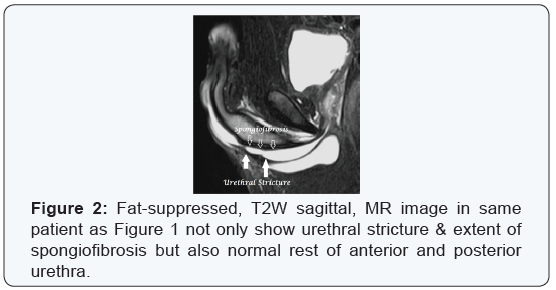
Although role of MRU in evaluation of MUS was first introduced in last decade of 20th century yet it did not gain significance until recent studies that revealed its high accuracy in delineating the location & length of male urethral strictures as well as presence & extent of spongiofibrosis together with other information that may be useful from management point of view like presence of urethral calculus, sinus or fistula, diverticulum, etc. (Figure 2) [11,12]. MRU is not only radiation-free & relatively non-invasive like SUG but also overcomes its major limitation by being highly reproducible and helpful in delineating posterior urethra & its axis in distraction injuries [1].
However in spite of having so many advantages, MRU has its demerits in the form of limited availability & expertise, expensive nature and higher examination time, in addition to claustrophobia and presence of cochlear implants & non-MRI compatible pacemaker [11,12]. In a study by El-Ghar et al [1], sensitivity, specificity & overall accuracy of RGU in anterior urethral strictures was reported to be 91%, 90% & 90%, respectively and for posterior stricture, it was 89%, 91.7% and 90%, respectively. However, on SUG, though all cases of anterior urethral strictures were detected with 100% accuracy yet for cases of posterior urethral stricture, the overall accuracy was only 60%. MRU diagnosed all the cases of anterior & posterior urethral strictures in the above study with exact delineation of their length except one case of normal caliber was diagnosed falsely at MR as anterior short segment urethral stricture leading to an overall sensitivity of 100%, specificity of 91.7% & accuracy of 95%.
Conclusion
To summarize, though RGU, VCUG & SUG in combination may provide sufficient clinical information in case of male urethral strictures to decide future course of management yet MRU can serve as single-stop shop giving the best possible information from imaging that can be utilised for best management. However, the decision of using MRU or other imaging modalities should be made taking in to consideration the clinical condition; time, technique & expertise available and financial viability.
References
- Mohamed Abou El-ghar, Yasser Osman, Elsayed Elbaz, Huda Refiae, Tarek El-Diasty (2010) MR urethrogram versus combined retrograde urethrogram and sonourethrography in diagnosis of urethral stricture. European Journal of Radiology 74: e193-e198.
- Yasser Osman, Mohamed Abou El-Ghar, Osama Mansour, Huda Refaie, Tarek El-Diasty (2006) Magnetic resonance urethrography in comparison to retrograde urethrography in diagnosis of male urethral stricture: is it clinically relevant? European Urology 50(3): 587-594.
- Tarek Khalaf Fath El-Bab, Amr Mohamad Abdelhamid, Ehab Mohamad Galal and Mohammed Farghally Amin (2013) Magnetic resonance urethrography versus conventional retrograde urethrography for diagnosis of anterior urethral stricture. Journal of American Science 9(9): 238-242.
- Sakti Das (1992) Ultrasonographic evaluation of the urethral stricture disease. Urology 40(3): 237-242.
- Narumi Y, Hricak H, Armenakas NA, Dixon CM, McAninch JW (1993) MR imaging of traumatic posterior urethral injury. Radiology 188(2): 439-443.
- Kawashima A, Sandler CM, Wasserman NF, LeRoy AJ, King BF Jr, et al. (2004) Imaging of urethral disease: a pictorial review. Radiographics 24(1): 195-216.
- MacDonald MF, Santucci RA (2005) Review and treatment algorithm of open surgical techniques for management of urethral strictures. Urology 65: 9-45.
- RK Rauniyar, CS Agrawal, MK Gupta, K Ahmad, A Gupta, et al. (2013) Comparative Study of Sonourethrography and Radiographic Urethrography in Urethral Lesions. NJR 3(4): 33-39.
- Shyam Manoharlal Talreja, Vinay Tomar, Sher Singh Yadav, Usha Jaipal, Shivam Priyadarshi, et al. (2016) Comparison of sonoelastography with sonourethrography and retrograde urethrography in the evaluation of male anterior urethral strictures. Turk J Urol 42(2): 84-91.
- Mitterberger M, Christian G, Pinggera GM, Bartsch G, Strasser H, et al. (2007) Gray scale and color Doppler sonography with extended field of view technique for the diagnostic evaluation of anterior urethral strictures. J Urol 177: 992-997.
- Deuk Jae Sung, Yun Hwan Kim, Sung Bum Cho, Yu Whan Oh, Nam Joon Lee, et al. (2006) Obliterative urethral stricture: MR Urethrography versus conventional retrograde urethrography with voiding Cystourethrography. Radiology 240: 842-848.
- Tarek Khalaf Fath El-Bab, Ehab Mohamad Galal, Amr Mohamad Abdelhamid, Mohammed Farghally Amin (2015) Magnetic resonance urethrography versus conventional retrograde urethrography in the evaluation of urethral stricture: Comparison with surgical findings. The Egyptian Journal of Radiology and Nuclear Medicine 46(1): 199-