




Research Article
Incidence and Prevalence of Anxiety, Depression, and Post-Traumatic Stress Disorder Among Critical Care Patients, Families, and Practitioners
Michael J Jacka1*, Nicholas Mitchell2 and Jorge Perez-Parada3
1Anesthesiology and Critical Care, University of Alberta, USA
2Department of Psychiatry, University of Alberta, USA
Submission: February 18, 2016; Published: April 29, 2016
*Corresponding author: Michael J Jacka, Anesthesiology and Critical Care, 8th Fl CSB, WCM HSC, University of Alberta, Edmonton AB T6G 2B7,8; Email: mjacka@ualberta.ca
How to cite this article: Michael J J, Nicholas M, Jorge P-P. Incidence and Prevalence of Anxiety, Depression, and Post-Traumatic Stress Disorder Among Critical Care Patients, Families, and Practitioners. J Anest & Inten Care Med. 2016; 1(1) : 555555. DOI: 10.19080/JAICM.2015.01.555555
Abstract
OBackground: WAnxiety, depression, and post-traumatic stress disorder (PTSD) are common complications of critical illness. Their prevalence is known to be higher among patients than among the general population. Little is known about their prevalence among families and among critical care staff.
Setting: Igeneral systems intensive care unit in a tertiary care university hospital
Methods: We measured the features of PTSD, anxiety, and depression using validated scales (PSS-SR, Zung anxiety scale, and PHQ-9 respectively), employing an anonymous survey of sequential consenting patients admitted with critical illness, their associated family next-of-kin (NOK), and members of the clinical staff involved (medical, nursing, and allied health). Survey was administered to patients and NOK at 28 days after ICU discharge, and to staff at patient admission.
Results: 30 patients, next-of-kin, and associated medical/nursing/allied health staff were approached. Participants included 60%, 50%, and 58% of eligible patients, NOK, and staff respectively. Among patients, NOK, and staff respectively, features consistent with the diagnoses of PTSD (50%, 33%, 19%), anxiety (61%, 33%, 41%), and depression (39%, 20%, 16%) were observed, substantially higher than expected based on population prevalence estimates.
Background
A critical illness is a life-threatening event that induces an intense response in its victim. Common, primordial responses to imminent threats to life include fear and anger. Sadness, also a basic emotion, intervenes concurrent with a sense of loss, whether acute or chronic. Long term adverse sequelae after exposure to intense life-threatening events include anxiety, depression, and post-traumatic stress disorder (PTSD). Not surprisingly, these conditions occur more frequently among critical care survivors than among the rest of the population. Less is known about the incidence and prevalence of these conditions among the families of critical care survivors and among critical care practitioners [1-11].
Anxiety is characterized by excessive and usually irrational concern about erstwhile non-threatening events or possible events that is disruptive because it interferes with normal social or economic function. It is distinguished from fear, a basic human emotion, in that fear is directed at a realistic threat e.g. imminent death during a critical illness. The life-time prevalence of anxiety in the general population is approximately 10%. Generalized anxiety disorder is described in the Diagnostic and Statistical Manual IV as including three or more symptoms of restlessness, difficulty with sleep, irritability, difficulty concentrating, or muscle tension in response to normal stressors, and that interfere with usual function.
Depression similarly has a life-time population prevalence of approximately 10%. As a major mood disorder, its diagnostic features include significant variations in appetite, sleep, concentration, and interactions with others, that interfere with usual social and economic function.
PTSD is a mood disorder that is related to both depression and anxiety, including features of each. The most distinct feature of PTSD is its beginning with a traumatic event or series. Other features include intrusive thoughts in relation to the traumatic event that interfere with normal function, avoidance of scenarios or places that may facilitate recall of the instigating event, and biologic manifestations of a stress response such as sweating, tachypnea, tachycardia, and flushing.
We sought to evaluate the incidence of anxiety, depression, and PTSD among critical care survivors and their families, and the prevalence of these among critical care practitioners. Our objective was to determine whether these conditions occurred at a different frequency compared to the non-critically ill population and their families, and if so which of them was most frequent.
Methods
The University of Alberta Hospital is a tertiary care centre, within which the General Systems ICU (GSICU) includes 28 beds for patients with medical, surgical, and traumatic critical illness. After institutional approval, we conducted a survey of patients (survivors), their families (immediate next-of-kin (NOK)), and the providers involved in their care..
In June 2012, thirty consecutive unselected surviving ICU patients and their NOK were approached and invited to provide informed written consent for this investigation. Staff members were invited to participate on the basis of providing care to the participating patients at the time of their admission to the ICU. Invited participating staff included the nurse, respiratory therapist, resident, dietician, pharmacist, physiotherapist, and attending staff for each patient. Staff members were limited to participating once.
The survey was delivered to patients and their NOK at 28 days after ICU discharge, either using the standard postal service if the patient had been discharged or transferred, or via hand delivery if the patient remained in hospital. Surveys were contained within a stamped self-addressed return envelope that did not include personal identifiers. Surveys were delivered to staff using hospital mail, using the same method of stamped selfaddressed return envelope. The investigation was announced and described to providers, who were advised of the study methods. Provider consent was implied by survey completion, and surveys did not include identifying information.
The survey consisted of three combined scales, and nonidentifying demographic descriptors. To assess the presence of anxiety and depression, we used the Zung self-reported anxiety scale and the patient depression questionnaire (PHQ- 9) respectively. PTSD was assessed using the post-traumatic symptom scale (PSS-SR). Using the Zung scale, anxiety was defined as a score of greater than 15. Depression was defined as a score of greater than 15 on the PHQ-9. PTSD was defined as a score of greater than 17 on the PSS-SR scale. Each of these scales has been validated independently and shown to provide good inter-rater and intra-rater reliability and validity [12-17].
Results
Of 30 patients and NOK approached, 18 patients (60%) and 15 NOK (50%) responded. Of ICU staff, 30 nurses, 5 respiratory therapists, 2 dieticians, 2 physiotherapists, 2 pharmacists, 8 resident physicians and 6 attending physicians were invited to participate. Responses were received from 20 nurses (67%), 3 respiratory therapists (60%), 6 resident physicians (75%), and 3 attending physicians (50%). No responses were received from dieticians, physiotherapists, or pharmacists. The subsequent results are based on the total of 65 responses received (overall response rate 57%).
Considering Table 1, among patients participating after surviving a critical illness, 50% met diagnostic criteria for PTSD at 28 days after ICU discharge using the screening questionnaire PSS-SR. This was also observed among 33% of the participating NOK and among 19% of staff.
Also in Table 1, anxiety was present according to the Zung scale among 61% of participating surviving patients and among 33% of the participating NOK. Anxiety was present among 41% of critical care staff.
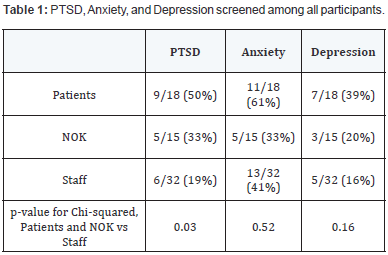
With regard to depression as measured by the PHQ-9, this was present among 39% of participating surviving patients and was present among 20% of their NOK. Depression was present among 16% of participating staff.
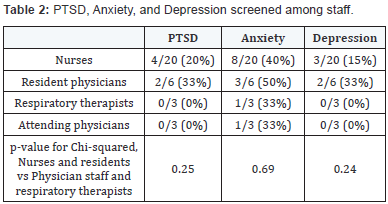
In Table 2, the presence of PTSD, anxiety, and depression was considered among participating staff according to staff category (e.g. nurse, physician, etc.). Symptoms of each of PTSD, anxiety, and depression were more common among participating nursing staff and resident physicians than among participating respiratory therapists and attending physicians. It was previously noted that none of the invited physiotherapists, pharmacists, and dieticians participated in the survey, and no conclusions can be drawn about these groups.
Discussion
The critical care unit in any hospital admits patients with the greatest degree of physiologic disturbance and greatest threat to life of patients in the hospital. The threat to life can leave survivors and their NOK with persistent residual disturbances in mood as a consequence of that threat. Constant exposure to patients and NOK under threat to life may also be associated with mood disturbance among bedside staff.
In this survey, we discovered that the prevalence of each of PTSD, anxiety and depression were substantially higher among patients, NOK, and staff than would have been expected based on the general population prevalence of these conditions. While detection of these mood disorders in ICU survivors and NOK has been reported in the literature [1-11], this study represents possibly one of the first that describes these conditions among ICU staff. Further exploration of the causes and consequences of these relatively increased incidences and prevalence, as well as attention to prevention and treatment, may be appropriate.
Each of PTSD, anxiety, and depression are disorders that can occupy a spectrum of implications on those with these conditions ranging from mildly inconvenient to debilitating. Socially, their recognition continues to carry varying levels of stigma that may further reduce both their perceived prevalence and reported significance. Consequently, the social burden of these conditions may be substantially greater than measured in studies such as this [12-13].
While we detected relatively increased prevalence of these conditions among surviving patients and NOK, we were unable to measure the duration of the conditions. Further investigation to determine duration of these disorders would be appropriate.
We did not have the medical nor nursing resource to address the effectiveness of possible preventive or therapeutic manoeuvres. While we did advise participants to contact their family physicians in event of concerns, we did not wish to raise expectation bias in survey completion by emphasizing therapeutic options.
The therapies available for these conditions range from cognitive behavioural therapy to pharmaceutical. In the most severe scenarios, patients may be treatment-resistant and debilitated. Consequently, identification of preventive strategies may be beneficial [12-18].
The higher prevalence of these disorders among nursing staff and resident physicians is somewhat in keeping with other findings in the literature showing higher prevalence of such conditions among first-responders to critical events. First-responders have less ability to remove themselves from exposure to events that are life-threatening to patients, and may suffer from internalization of this exposure. On the other hand, attending staff and associated staff (e.g. pharmacists, dieticians) may be unaware of the significance of the perceived threats to life on bedside providers. A greater level of awareness of this may be appropriate for both first-responders and for those more removed from the moment-to-moment intensity.
This study was too small to evaluate association between severity of patient illness and its effect on immediate NOK or on immediate care givers. Further investigation could evaluate these hypotheses.
Considering the prevalence of these conditions among patients, it is noted that this was a sequential (cross-sectional) non-randomized survey that was done at 28 days after ICU discharge and was obviously limited to survivors. Administration of this survey later after discharge may have resulted in a different detected prevalence of these conditions. However, due to timing constraints, we were not able to include patients that were admitted during the study period and survived but that remained within the ICU due to severity of illness. These patients would likely have been exposed to greater threat, as would also have been the case for their NOK. A randomized design performed over a longer period of time may have achieved a different result, as the conclusions of this study may have been affected by timing of administration. Finally, the response rate (60%) among patients was reasonable to allow some generalization to the surviving non-responding patients. The response rate among NOK was slightly lower, and was limited to study of NOK of surviving patients. Interestingly, the response rate among staff was similar to that among patients, and is also probably appropriate for some generalization.
Within these limitations, the incidences of PTSD, anxiety, and depression were higher among patients and NOK, as well as among staff, than expected among the population at large. Consideration of further investigation to determine causes of these conditions in these groups, as well as to evaluate prevention, treatment, and long-term sequelae, would be appropriate.
References
- Dinholm CJ (2009) Coping strategies during hospitalization and recovery following motor vehicle trauma: A personal account. Clinical Psychologist 13(3): 116-121.
- Scragg P, Jones A, Fauvel N (2001) Psychological problems following ICU treatment. Anaesthesia 56(1): 9-14.
- Griffiths J, Fortune G, Barber V, Young JD (2007) The prevalence of post traumatic stress disorder in survivors of ICU treatment: a systematic review. Intensive Care Med 33(9): 1506-1518.
- Davydow DS, Gifford JM, Desai SV, Needham DM, Bienvenu OJ (2008) Post traumatic stress disorder in general intensive care unit survivors: a systematic review. General Hospital Psychiatry 30(5): 421-434.
- Kentish-Barnes N, Lemiale V, Chaize M, Pochard F, Azoulay E (2009) Assessing burden in families of critical care patients. CCM 375(10 Suppl): 448-456.
- Myhren H, Ekeberg O, Tøien K, Karlsson S, Stokland O (2010) Post traumatic stress, anxiety and depressive symptoms in patients during the first year post intensive care unit discharge. Crit Care 14(1): R14-R24.
- Wade DM, Howell DC, Weinman JA, Hardy RJ, Mythen MG, et al. (2012) Investigating risk factors for psychological morbidity three months after intensive care: a prospective cohort study. Critical Care 16(5): R192.
- Davidson JE, Jones C, Bienvenue OJ (2012) Family response to critical illness: Post intensive care syndrome – family. CCM 40(2): 618-624.
- Kross EK, Engelberg RA, Gries CJ, Nielsen EL, Zatzick D, et al. (2011) ICU care associated with symptoms of depression and post traumatic stress disorder among family members of patients who die in ICU. Chest 139(4): 795-801.
- Paparrigopoulos T, Melissaki A, Efthymiou A, Tsekou H, Vadala C, et al. (2006) Short-term psychological impact on family members of intensive care patients. J of Psychosomatic Research 61(5): 719-722.
- Kessler RC, Demler O, Frank RG, Olfson M, Pincus HA, et al. (2005) Prevalence and treatment of mental disorders 1990-2003. NEJM 352(4): 2515-2523.
- Katzman MA, Bleau P, Blier P, Chokka P, Kjernisted K, et al. (2014) Canadian clinical practice guidelines for the management of posttraumatic stress, anxiety, and obsessive-compulsive disorders. BMC Psychiatry 14(Suppl 1): 1-86.
- Spitzer RL, Kroenke K, Williams JBW (1999) Validation and utility of a self-report version of PRIME-MD. JAMA 282(18): 1737-1744.
- Zung WWK (1971) A rating instrument for anxiety disorders. Psychosomatics 12(6): 371-375.
- Kroenke K, Spitzer RL, Williams JBW (2001) The PHQ-9: Validity of a brief depression severity measure. J Gen Int Med 16(9): 606-613.
- Sin GL, Abdin E, Lee J (2012) The PSS-SR as a screening test for PTSD in first-episode psychosis patients. Early Interv Psychiatry 6(2): 191- 194.
- Foa EB, Riggs DS, Dancu CV, Rothbaum BO (1993) Reliability and validity of a brief instrument for assessing post-traumatic stress disorder. J of Traumatic Stress 6(4): 459-474.
- Peris A, Bonizzoli M, Iozzelli D, Migliaccio ML, Zagli G, et al. (2011) Early intra-intensive care unit psychological intervention promotes recovery from post traumatic stress disorders, anxiety, and depressive symptoms in critically ill patients. Crit Care 15: R41-R49.