




Hemangioma of Internal Auditory Canal: Systemic Review
Omar Ramadan*
Department of ENT, USA
Submission: October 15, 2016; Published: October 25, 2016
*Corresponding author: Omar Ramadan, Independent researcher, ENT registrar, Paterson NJ, New Jersey, USA
How to cite this article: Omar R. Hemangioma of Internal Auditory Canal: Systemic Review. Glob J Otolaryngol. 2016; 2(2): 555585. DOI: 10.19080/GJO.2016.02.555585
Abstract
Objectives: The objective of this study was to present a review article about internal auditory canal hemangioma.
Data Sources: Published English-language literatures.
Review Methods: We included studies about internal auditory canal hemangioma.
Results: 42 studies were included in this study. The results showed that most patients were male, the age of patients varied between 5 to 69 years old. Two cases were multiple familial hemangioma, while the most other cases were sporadic. Hearing loss was the most common symptoms, 37% patients had facial palsy, and 38% patients had vestibular symptoms. Since most patients had non- serviceable hearing loss so, translabrynithine approach was the most common surgical approach. Most serviceable hearing patients lost their serviceable hearing after surgery. Only one third of patients with facial palsy had improvement after surgery. Most cases had attachment to facial nerve and can be removed totally.
Conclusion: we should suspect IAC hemangioma in any patient with considerable hearing loss and facial palsy with small lesion in internal auditory canal.
Keywords: IAC: Internal Auditory Canal; Cavernous hemangioma; Facial spasm; Translabrynithin
Abbreviations: TL: Translabrynthine; RS: Retrosigmoid; MFA: Middle Fossa Approach; IAC: Internal Auditory Canal; TR: Total Removal; NTR: Near Total Removal; HL: Hearing Loss; FP: Facial Palsy
Introduction
Cavernous hemangioma of the internal auditory canal (IAC) is a rare disease. It comprises 10 to 20% of all central nervous vascular malformations. They are composed of large, sinusoidal, thin-walled capillary spaces that may invade the surrounding neural tissue. They can mimic the symptoms of vestibular shwannomas. We review the clinical features and the management of the IAC hemangioma [1].
Material and Methods
Literature review was conducted using PubMed (MEDLINE) and Google Scholar for English articles, the following keywords were used: internal; auditory; canal and hemangioma.
Inclusion Criteria
All internal auditory canal hemangioma articles published after 1975 were included in the study.
Results

Demographic
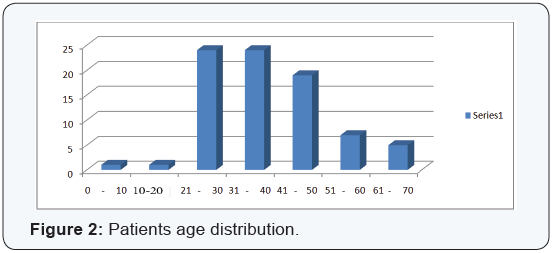
There were 81 patients of age ranged from 5 to 69 with majority of the patients between 20 to 50 year old. There were 57 males and 24 females in the study (Figures 1 & 2).
Symptoms
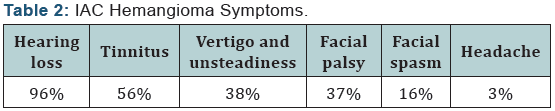
78 patients had hearing loss (96%). 11 patients of them had sudden hearing loss (14%), while the other 67 patients had progressive hearing loss (86%). 16 patients had serviceable hearing loss (20%), while the other 52 patients had nonserviceable hearing a loss (80%).
46 patients had tinnitus (56%), 31 patients had vestibular symptoms (38%) (16 patients had vertigo and 15 patients had unsteadiness). 30 patients had facial palsy (37%), 6 patients of them had sudden facial palsy (20%), 3 patients of them had recurrent facial palsy (10%), while the other 21 had progressive facial palsy (70%). 13 patients had facial spasm (16%). 2 patients had headache (3%), and 2 patients had familial multiple hemangioma (3%) (Table 2).
Management
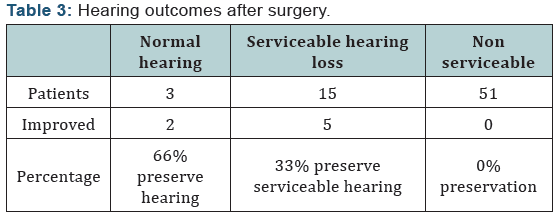
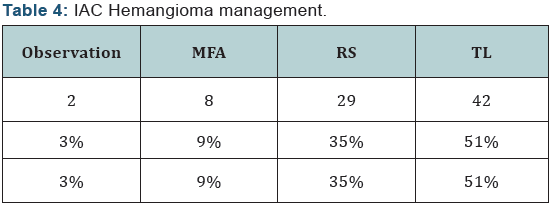
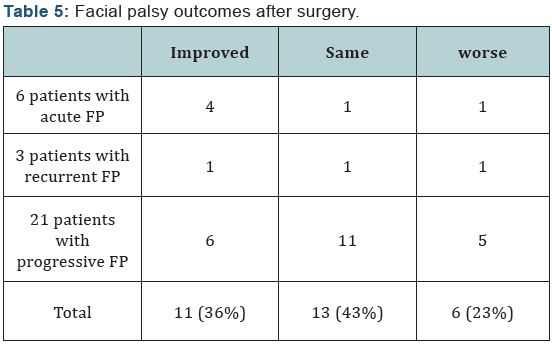
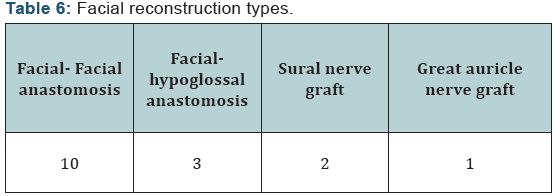
Two patients were managed by observation. 79 patients had a surgery, 3 of them had normal hearing, and 15 patients of them had serviceable hearing loss, while the other 51 patients had non-serviceable hearing loss (Table 3). Only 11 articles reported the postoperative clinical progress of vestibular symptoms, and all reported patients with vestibular symptoms improved. 13 patients had preoperative facial spasm, and it disappeared in all of them postoperatively. Two patients were managed conservatively, 8 patients had MFA, and 29 patients had RS approach, while the other 42 patients had TR approach (Table 4). 30 patients with facial palsy had a surgery, 11 patients of them had facial weakness improvement (Table 5). 16 patients had facial reconstruction (20%) (Table 6). 68 patients had a limited disease to IAC, while 13 patients had disease extension
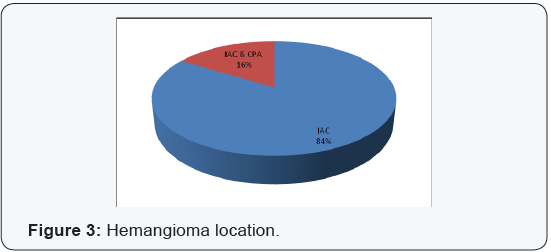
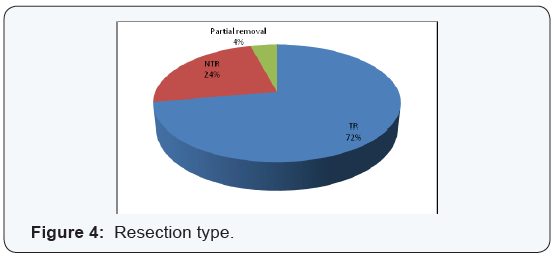
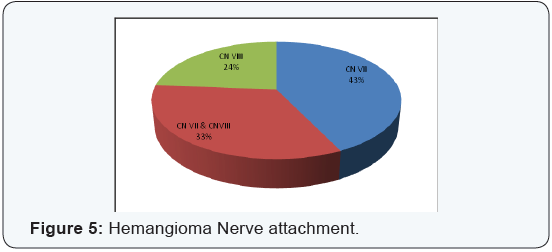
into CPA (Figure 3). 72 articles reported the surgical removal type, 52 patients of them had a total surgical resection, and 17 patients of them had a near total resection while the other 3 patients had only partial resection (Figure 4). Hemangioma attachments were reported in 63 patients, 27 patients of them had CN VII attachment, and 21 patients of them had CN VII & CN VIII attachment, while the other 15 patients had CN VIII attachment (Figure 5).
Results
Most patient were male with age ranging between 20 to 50 years old. Most patients had non-serviceable hearing loss.38% patients had vestibular symptoms, 37% patients had facial palsy, 16% patients had facial spasm. Only third patient with serviceable-hearing loss preserved their hearing abilities after surgery, third patient with facial palsy had significant improvement after surgery (acute facial palsy has a better prognosis than progressive facial palsy), and all patients with facial spasm and vestibular symptoms had a good improvement. Most cases were located primary to IAC, most cases had attachment to facial nerve and can be removed totally, and about20% of patients had facial reconstruction surgery due to advanced facial nerve involvement.
Conclusion
IAC hemangioma is a rare disease with poor outcomes prognosis, we should suspect this disease in patients with progressive hearing loss and facial palsy with small lesion in internal auditory canal vertigo and Tinnitus.
Discussion
Vestibular schwannoma is the most common tumor in IAC and the cerebellopontine angle (CPA). Other tumor lesions of CPA area include meningioma, primary cholesteatoma, facial nerve neuroma, various vascular tumors, metastatic tumors, and others. Cavernous angioma was reported rarely in the IAC. Sundares et al. reported the first case of IAC cavernous angioma in 1976. These tumors were considered to originate from the capillary bed of the epineurium nerve. Vascular steal mechanism in which the blood is taken by tumor instead of the nerve causing nerve function loss even with a small size of tumor. Histopathologically, they consist of large thin-walled blood vessels that lined by flattened endothelium, which stain positive by endothelial marker CD 31, the stroma is composed of fibrous component and has mainly myofibroblast and fibroblast that stain positive for smooth muscle actin.
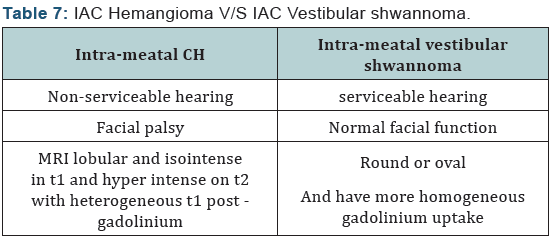
Depending on nerve origin and location, these tumors can cause severe progressive or sudden sensorineural hearing loss, tinnitus, sudden or progressive facial nerve palsy, facial spasm, vertigo and disequilibrium even when they are in small size. The tumor size is usually less than 10 mm. On CT scan, IAC hemangioma appear as iso-or hyper- dense lesion with slight enhancement after intravenous administration of contrast, usually stippled calcifications could also be seen with enlargement of the IAC. On MRI, It appears as lobular and isointense in T1 and hyperintense on T2 with heterogeneous T1 post - gadolinium enhancement. The main differential diagnosis is IAC Vestibular shawanoma (Table 7). Other differential diagnosis may include meningioma, lipoma, melanoma, hamartoma, and lymphoma.
Complete surgical resection with avoiding complications such bleeding is the goal of treatment. Radiotherapy may promote growth and hemorrhage, so it is not recommended. No symptomatic cases can be managed conservatively. Symptomatic case should be resected surgically. Surgical approach is depended on hearing deficit and tumor size. Translabyrinthine approach is recommended for patient with non-serviceable hearing loss. Middle fossa approach and retrosigmoid approach are recommended for patients with serviceable hearing loss. This lesion could be attached firmly with facial nerve. Since the tumor is benign and slow growing, it is advocated to perform a near total resection in case where the tumor is difficult to dissect from facial nerve [18,26,27].
Acknowledgement
Dana Library , Clifton memorial library and Mrs. Patricia May.
Conflict of interest
Author declared no conflict of interest
References
- Sundaresan N, Eller T, Ciric I (1976) Hemangiomas of the internal auditory canal. Surg Neurol 6(2): 119-121.
- Mangham CA, Carberry JN, Brackmann DE (1981) Management of intratemporal vascular tumors. Laryngoscope 91(6): 867-876.
- Pappas DG, Schneiderman TS, Brackmann OF, Simpson SC, Chandra Sekar B, et al. (1989) Cavernous hemangiomas of the internal auditory canal. Otolaryngol Head Neck Surg 101(1): 27-32.
- Madden GJ, Sirimanna KS (1990) Cavernous hemangioma of the internal auditory meatus. J Otolaryngol 19(4): 288-291.
- Bordi L, Pires M, Symon L, Cheesman AD (1991) Cavernous angioma of the cerebello-pontine angle: a case report. Br J Neurosurg 5(1): 83-86.
- Jacobson J, Reams C (1991) Neurotologic disease in four patients with normal audiometric findings. Am J Otol 12(2):114-118.
- Cremers WR, Theunissen EJ, Thijssen HO, Meijer H, Faverly D (1991) Cavernous hemangioma of the internal acoustic canal. Am J Otol 12(5): 370-373.
- Fujino A, Tokumasu K, Yoshio S, Momiyama Y, Nakayama M (1993) A case of cavernous hemangioma in the internal auditory canal. Auris Nasus Larynx 20(4): 303-308.
- Babu R, Ransohoff J, Cohen N, Zagzag D (1994) Cavernous angiomas of the internal auditory canal: a case report and review of the literature. Acta Neurochirurgica (Wien) 129(1): 100-104.
- Kohan D, Downey LL, Lim J, Cohen NL, Elowitz E (1997) Uncommon lesions presenting as tumors of the internal auditory canal and cerebellopontine angle. Am J Otol 18(3): 386-392.
- Saleh E, Naguib M, Russo A, Taibah AK, Sanna M (1993) Vascular malformation of the internal auditory canal. J Laryngol Otol 107(11): 1039-1042.
- Greiner-Perth R, Schenke H, Neubauer U (1997) Cavernous malformation of the internal auditory canal. Acta Neurochirurgica (Wien) 139(11): 1090-1091.
- Fukuda Y, Ganança FF, Nascimento LA, Testa JR, Munhoz MS, et al. (1995) Cavernous hemangioma of the internal auditory canal. Apropos of a case. Rev Laryngol Otol Rhinol (Bord) 116(3): 229-230.
- Gjuric M, Koester M, Paulus W (2000) Cavernous hemangioma of the internal auditory canal arising from the inferior vestibular nerve: case report and review of the literature. Am J Otol 21(1): 110- 114.
- Sasaki T, Sasaki T, Okamoto K, Ishida T, Kirino T (1999) Cavernous angioma of the internal acoustic meatus-case report. Neurol Med Chir (Tokyo) 39(12): 847-851.
- Omojola MF, al Hawashim NS, Zuwayed MA, al Ferayan A (1997) CT and MRI features of cavernous haemangioma of internal auditory canal. Br J Radiol 70(839): 1184-1187.
- https://www.ncbi.nlm.nih.gov/pubmed/9696889?dopt=Abstract
- Samii M, Nakamura M, Mirzai S, Vorkapic P, Cervio A (2006) Cavernous angiomas within the internal auditory canal. J Neurosurg 105(4): 581-587.
- https://www.ncbi.nlm.nih.gov/pubmed/17235534?dopt=Abstract
- Safronova MM, Vaz AR, Resende M, Pereira JR, Honavar M, et al. (2009) Cavernous malformation of the internal auditory canal: a diagnostic challenge. Otol Neurotol 30(7): 1015-1017.
- Jose E Barrera, Herman Jenkins, Sherif Said (2004) Cavernous hemangioma of the internal auditory canal: a case report and review of the literature. American Journal of Otolaryngology 25(3): 199-203.
- Aquilina K, Nanra JS, Brett F, Walsh RM, Rawluk D (2004) Cavernous angioma of the internal auditory canal. J Laryngol Otol 118(5): 368- 371.
- Alobid Islam, Gastón Felix, Morello Antonio, Menéndez Luis Miguel, Benítez Pedro (2002) Cavernous haemangioma of the internal auditory canal. Acta Otolaryngol 122(5): 501-503.
- https://www.ncbi.nlm.nih.gov/pubmed/10962680?dopt=Abstract
- Sepehrnia A, Rebolledo Godoy AP, Reusche E (2000) A cavernous hemangioma simulating an intracanalicular acoustic neurinoma. A case report. Zentralbl Neurochir 61(4): 194-197.
- Zhu WD, Huang Q, Li XY, Chen HS, Wang ZY, et al. (2016) Diagnosis and treatment of cavernous hemangioma of the internal auditory canal. J Neurosurg 124(3): 639-646.
- Oldenburg MS, Carlson ML, Van Abel KM, Giannini C, Jacob J, et al. (2015) Cavernous hemangiomas of the internal auditory canal and cerebellopontine angle. Otol Neurotol 36(1): e30-34.
- Mastronardi L, Carpineta E, Cacciotti G, Di Scipio E, Roperto R (2016) Cavernous hemangioma of the internal auditory canal encasing the VII and VIII cranial nerve complex: case report and review of the literature. Neurosurg Rev 39(2): 349-354.
- Hanamitsu M, Okumura K, Yazawa Y, Fukui J, Suzuki M (2004) Cavernous haemangioma of the internal auditory canal: a case report. J Clin Neurosci 11(3): 337-340.
- Bonfort G, Veillon F, Debry C, Kehrli P, Chibbaro S (2015) VIIIth nerve cavernous hemangioma mimicking a stage 1 acoustic schwannoma. Neurochirurgie 61(5): 352-355.
- Nakashima T, Kawano H, Matsuda K, Tono T (2012) Hemangioma of the internal auditory canal: Case report. Otol Jpn 22(5): 838-843.
- http://acta.tums.ac.ir/index.php/acta/article/view/225
- Silveira RL, Andrade GC, Pinheiro Júnior N, Pittella JE, Barbosa VC (2015) Cavernous hemangioma of the internal auditory canal encasing the VII and VIII cranial nerve complex: case report. Arq Neuropsiquiatr 63(1): 163-165.
- Giuseppe Magliulo, Giannicola Iannella, Simone Alessi, Massimo Re (2014) Meatal segment of facial nerve and cavernous angioma. Annals of Otolaryngology and Rhinology 1(1): 1004.
- Mahran A, Samii M, Penkert G, Ostertag H (1991) Vascular Lesions of the Internal Auditory Canal. Skull base surgery 1(2): 78-84.
- Sepehrnia A, Rebolledo Godoy AP, Reusche E (2000) A cavernous hemangioma simulating an intracanalicular acoustic neurinoma. A case report. Zentralbl Neurochir 61(4): 194-197.
- Refass A, Bozorg Grayeli A, Bouccara D, Ismail M, Cyna-Gorse F, et al. (2006) Atypical haemangioma of the internal auditory meatus: a case report. Eur Arch Otorhinolaryngol 263(7): 627-631.
- Matias-Guiu X, Alejo M, Sole T, Ferrer I, Noboa R, et al. (1990) Cavernous angiomas of the cranial nerves. Report of two cases. J Neurosurg 73(4): 620-622.
- http://link.springer.com/article/ 10.1007%2FBF01105784
- Feng Shao-Yan, Fan Yun-Ping, Chen Shulin, Hong Hai-Yv, Zhang Zhi- Gang (2012) Cavernous hemangioma of the internal auditory canal: a case report. Int Adv Otol 8(3): 470-474.
- Moore GF, Johnson PJ, McComb RD, Leibrock LG (1995) Venous hemangioma of the internal auditory canal. Otolaryngol Head Neck Surg 113(3): 305-309.
- Omar H Ahmed, Eric W Cerrati, David R Friedmann, Matija Snuderl, Mari Hagiwara, Daniel Jethanamest (2016) Intracanalicular Venous Malformation of the Internal Auditory Canal. New York University Langone Medical Center 1: 128.
- Shim HJ, Song DK, Lee SW, Lee DY, Park JH, et al. (2007) A case of unilateral sensorineural hearing loss caused by a venous malformation of the internal auditory canal. Int J Pediatr Otorhinolaryngol 71(9): 1479-1483.
- Di Rocco F, Paterno V, Safavi-Abbasi S, El-Shawarby A, Samii A, et al. (2006) Cavernous malformation of the internal auditory canal. Acta Neurochir (Wien) 148(6): 695-697.















