




Electroacoustic Stimulation with Cochlear Implants for Deafness Treatment
João Paulo Peral Valente1, Luciane Calonga2, Alexandre Caixeta Guimarães1, Walter Adriano Bianchini1 , Jorge Rizzato Paschoal1 and Guilherme Machado de Carvalho1*
1Department of ENT, Campinas University, South America
2Department of Audiologist, Cochlear Implant Specialist, South America
Submission: July 09, 2016; Published: August 05, 2016
*Corresponding author: Guilherme Machado de Carvalho, Head & Neck Surgery Department, UNICAMP, PO Box 6111, Postal Code: 13081-970, São Paulo, Brazil, South America.
How to cite this article: Guilherme M dC, João P PV, Luciane C, Alexandre CG, Walter A B, et al. Electroacoustic Stimulation with Cochlear Implants for Deafness Treatment. Glob J Oto. 2016; 1(5): 555572. DOI: 10.19080/GJO.2016.01.555572
Abstract
Background: Cochlear implant is an electronic hearing aid surgically inserted into the inner ear that, unlike a conventional hearing aid, picks up sound waves and transforms it into an electrical impulse that directly stimulates the cochlear nerve.
Objective: This study aims to describe the profile and outcomes of patients submitted to hybrid cochlear implant in the in a tertiary hospital in the last three years.
Methods: It was conducted a clinical study including 8 patients implanted with the brand MED-EL FLEX EAS in a tertiary hospital in the last three years.
Results: It was observed an improvement in all tonal thresholds after the activation of the cochlear implant.
Conclusion: The hybrid cochlear implant was successful procedure, with an improvement of tonal thresholds after the activation of cochlear implants..
Keywords: Cochlear implants; Hearing aids; Hearing preservation; Electroacoustic stimulation; Deafness; Bilateral deafness
Introduction
Cochlear implant is an electronic hearing aid surgically inserted into the inner ear that, unlike a conventional hearing aid, picks up sound waves and transforms it into an electrical impulse that directly stimulates the cochlear nerve. The development of multichannel cochlear implants, new speech processing strategies and more modern processors enabled gradually better results. In 1995, most of the implanted patients already reached results above 80% correct sentences in speech perception tests [1,2]. With the improvement of the cochlear implant performance, studies began to be developed to carry out cochlear implant in patients with residual hearing, which were not good fit with hearing aids.
New types of electrodes and changes in surgical technique have been developed in order to preserve the auditory trace these patients and promote rehabilitation by means of electrical stimulation combined with the acoustic stimulation (soft surgery) [3-7]. The electro-acoustic stimulation (EAS) of hearing aims to combine the amplification of residual hearing of the patient by conventional hearing aids, with electrical stimulation of the cochlea performed by the cochlear implant [8]. This is the principle of hybrid cochlear implants. This study aims to describe the profile and outcomes of patients submitted to hybrid cochlear implant in a tertiary hospital in the last three years.
Methods
It was conducted a clinical study including 8 patients implanted with the brand MED-EL FLEX EAS in a tertiary hospital in the last three years. Were admitted to the study all patients in the last three years whose implant was done with full insertion of the electrode bundle and consented to participate in the study through the Term of Consent. All patients used the internal component SONATA TM model and have been adapted by Maestro System TM software. Patients who had postoperative electro stimulation used speech processor DUET 2 Tim. The group had purely electrical stimulation postoperative differed only in the speech processor, having been used in such cases the OPUS 2 Tim. Patients with incomplete data, which did not meet the inclusion criteria or who would not be subject to such assessment were excluded from this Protocol.
Audiological evaluation
Audiological tests were performed including impedanciometry, speech and pure tone audiometry. The tests were performed using an audiometer AC30-SD25, calibrated according to ISO 389 standards / 64. The OAEs distortion products were performed at frequencies 700 to 8000 Hz with stimulus at 65-55 dB SPL, with a frequency ratio of 1.22. OEA was considered present when the signal/noise ratio was greater than 6 dB, and with reproducibility greater than or equal to 70%. The tests from the ABR and CM were performed with insert earphones. Stimulus of 100 dB HL was used for the ABR covered with frequencies between 250 and 8.000 Hz, with duration of 100 microseconds, and condensed and rarefied polarities. The abnormality of ABR was defined as absence of wave formation or severe changes in morphology of the same with up to 100 dB HL stimulus.
The CM was evaluated in tests from the ABR, with the feature of inverting the polarity (condensed and rarefied). When CM was positive with stimuli of 100 dB HL electrophysiological threshold, in decreasing order was researched. For ABR, which were repeated at least two times, the device AT-235 (Interacoustics) was used. Hearing loss impairment was classified through audiometry stratification in mild, moderate, severe / severe or profound hearing loss [9].
Speech perception tests: During preoperative evaluation, all subjects underwent to a speech perception test on the same day of their surgery. The speech perception test is based on several studies in English language, adapted and developed for Portuguese language by Bevilacqua et al. [10]. Patients performed the tests with hearing aids, in a quiet and peaceful place (best aided condition). Postoperatively, all subjects repeated the speech perception test at least one year experience with cochlear implant. The tests were performed using the cochlear implant (CI). The same audiologist performed all tests (pre-and postoperative).
Subjective evaluations: When the patients did their postoperative speech tests it were asked to rate the quality of their experience with CI compared to last year on a Likert scale ranging from 0 to 10, similar to the visual analog scale. A score of 0 indicates that user intervention regretted not recommend to others, and felt he / she had been better in the past, with their hearing aids. A score of 10 indicates that the user was completely satisfied with the work and highly recommended.
Statistical analysis
The data were analyzed using descriptive analysis, with production of means, medians, standard deviation tabs. Chi- Square was used to compare the groups of our sample. Because of the small size of some of the variables analyzed Fisher’s Exact test was also used to check the correlation between the groups. The confidence Interval was of 95%, and p-value <0.05 was considered significant.
Ethical considerations
The institutional review board approved this study and all subjects gave written informed consent. The survey was conducted considering ethical, and was approved by the Ethics Committee under protocol number 24802914.8.0000.5404.
Results
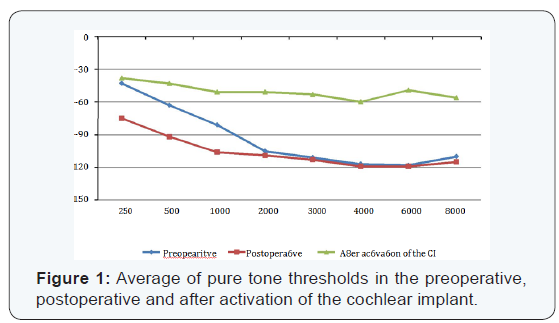
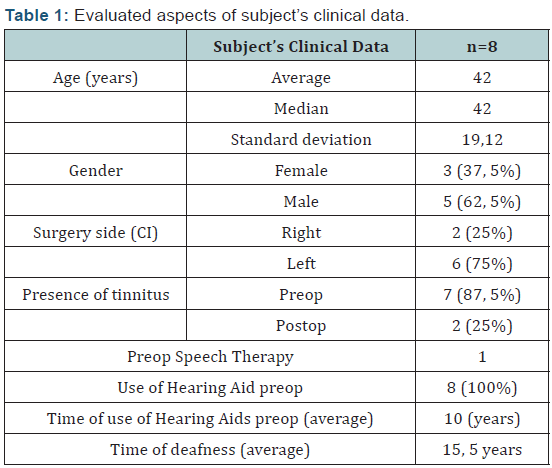
The hybrid cochlear implants were performed in 8 patients in these periods. The evaluated aspects are described in (Table 1). In (Figure 1) can be seen the average of pure tone thresholds in the preoperative, postoperative and after activation of the cochlear implant (CI).
Discussion
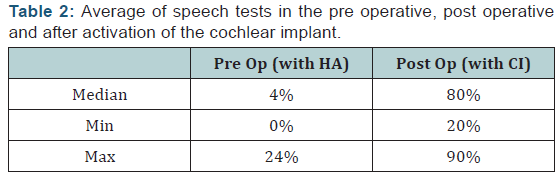
The EAS of hearing aims to combine the amplification of residual hearing of the patient by conventional hearing aids, with electrical stimulation of the cochlea performed by the cochlear implant. It is an excellent option for people with residual hearing in low frequencies (preserved below 1 kHz) but not at high frequencies and with insufficient benefit with hearing aids [8]. Typically, these individuals are able to detect all the vowels, but probably few or no consonants. The low frequencies also provide additional information for speech perception, speech production and perception of environment sounds. This preservation of residual hearing of low frequency despite the insertion of an electrode has become the cornerstone for the consolidation of this concept [6,7] (Table 2).
With the prospect of the combined EAS cochlear implant should not compromise the residual hearing. New prototype electrodes are therefore currently under development to ensure the preservation of hearing. Surgical measures to avoid trauma to the basal turn are of great importance in preserving residual hearing [11]. There are indications that the new prototype of the Med-El Flex electrode has good mechanical properties for the secure deployment and atraumatic: is highly flexible, especially on the edge of the area, producing no substantial trauma to the cochlea structures and is inserted using an appropriate surgical technique atraumatic [11]. The lack of anatomical trauma to the cochlear structures is necessary for the preservation of residual hearing of low frequency.
Several studies have demonstrated the superiority of bimodal stimulation EAS for patients with residual hearing who had preserved hearing about any other modality. These advantages were especially observed with increasing speech recognition, better perception in noisy environments, subjective improvements in sound quality when listening to music, and other situations [6,7,12-14]. Another multi centric clinical study demonstrated the effect of EAS in individuals with residual hearing of low frequency, both in speech perception and subjective quality [6,7]. The subjects were evaluated based on a series of audiological tests, and through a subjective questionnaire to assess the benefit of the hearing aid. Each subject underwent attempted hearing preservation cochlear using MED-EL electrode C40. Residual hearing ipsilateral and discrimination skills were evaluated at set intervals up to 12 months after the EAS. All subjects had a statistically significant benefit in all three tests speech perception over time. These significant benefits were also reflected in the subjective results of benefit by using the questionnaire. The worsening at tonal thresholds after the surgery is justified by the surgical trauma, but it was observed an improvement in all tonal thresholds after the activation of the cochlear implant. The hybrid cochlear implant was a successful procedure, with an improvement of tonal thresholds after the activation of cochlear implants.
Conclusion
The soft surgery was a successful procedure considering the improvement and preservation of tonal thresholds after the activation of cochlear implants, with no complications regarding the studied patients.
Acknowledgement
We would like to thank all patients and their families, medical residents, employees and all members of the ENT service.
References
- Eshraghi AA, Rodriguez M, Balkany TJ, Telischi FF, Angeli S, et al. (2009) Cochlear implant surgery in patients more than seventynine years old. Laryngoscope 119(6): 1180-1183.
- Olze H, Gräbel S, Förster U, Zirke N, Huhnd LE, et al. (2012) Elderly patients benefit from cochlear implantation regarding auditory rehabilitation, quality of life, tinnitus, and stress. Laryngoscope 122(1): 196-203.
- Orabi AA, Mawman D, Al-Zoubi F, Saeed SR, Ramsden RT (2006) Cochlear implant outcomes and quality of life in the elderly: Manchester experience over 13 years. Clin Otolaryngol 31(2): 116-122.
- Park E, Shipp DB, Chen JM, Nedzelski JM, Lin VY (2011) Postlingually Deaf Adults of All Ages Derive Equal Benefits from Unilateral Multichannel Cochlear Implant. J Am Acad Audiol 22(10): 637-643
- Balfour PB, Hawkins DB (1992) A comparison of sound quality judgements for monoaural and binau-ral hearing aid processed stimuli. Ear Hear 13(5): 331-339.
- Gstoettner W, Kiefer J, Baumgartner WD, Pok S, Peters S, et al. (2004) Hearing preservation in cochlear implantation for electric acoustic stimulation. Acta Otolaryngol 124(4):348-352.
- Gstoettner WK, van de Heyning P, O’Connor AF, Morera C, Sainz M, et al. (2008) Electric acoustic stimulation of the auditory system: results of a multi-centre investigation. Acta Otolaryngol 128(9):968-975.
- Arnoldner C, Lin VY (2013) Expanded selection criteria in adult cochlear implantation. Cochlear Implants Int 14(4): 10-13.
- Goodman A (1965) Reference zero levels for pure-tone audiometers. ASHA 7: 262-273.
- Bevilacqua MC, Banhara MR, Da Costa EA, Vignoly AB, Alvarenga KF (2008) The Brazilian Portuguese hearing in noise test. Int J Audiol 47(6): 364-365.
- Adunka O, Kiefer J, Unkelbach MH, Lehnert T, Gstoettner W (2004) Development and evaluation of an improved cochlear implant electrode design for electric acoustic stimulation. Laryngoscope 114(7):1237-1241.
- Kiefer J, Gstoettner W, Baumgartner W, Pok SM, Tillein J, et al. (2004) Conservation of low-frequency hearing in cochlear implantation. Acta Otolaryngol 124(3):272-280.
- Gantz BJ, Hansen MR, Turner CW, Oleson JJ, Reiss LA, et al. (2009) Hybrid 10 clinical trial: preliminary results. Audiol Neurootol 14(1): 32-38.
- Gfeller KE, Olszewski C, Turner C, Gantz B, Oleson J (2006) Music perception with cochlear implants and residual hearing. Audiol Neurootol 11(1): 12-15.















