




Pediatric Retropharyngeal Abscess
Sumit Sharma*
Department of ENT, Mayo Institute of Medical Sciences, India
Submission: July 15, 2016; Published: July 25, 2016
*Corresponding author: Sumit Sharma, Department of ENT, Royale Medical Centre, L 3/67, Sector-D, Near Happy World Girls College, Aliganj, Lucknow, 226024, Tel:9839178240; Email:entsumit@rediffmail.com
How to cite this article: Sumit S. Pediatric Retropharyngeal Abscess. Glob J Oto. 2016; 1(5): 555571. DOI: 10.19080/GJO.2016.01.555571
Abstract
Retropharyngeal abscesses are deep neck space infections that can pose an immediate life-threatening emergency, with potential for airway compromise and other catastrophic complications. Retropharyngeal abscess can lead to airway obstruction or sepsis - both life-threatening emergencies. Fatalities normally occur from patients not receiving treatment immediately and suffocating prior to knowing that anything serious was wrong. This is a retrospective study of five (5) cases with the discharge diagnosis of Retropharyngeal abscess treated in the past 3 years, only children below 12 yrs were taken in the study, the disease predominantly presented with fever and pain in throat with dysphagia, poor oral intake, neck pain and sore throat. Patients were immediately investigated by X-ray and CT scan, and once the diagnosis of retropharyngeal abscess was established, they were managed by aspiration under General Anesthesia, along with intravenous Antibiotics. Early diagnosis is the key to management of these conditions to avoid morbidity and mortality. Some interesting observations like incidence of Koch’s lesions and type of surgical intervention chosen along with possibility of recurrence will be presented in detail.
Keywords: Retropharyngeal abscess; Pediatric neck abscess; Neck swellings; Retropharyngeal buldge
Introduction
Retropharyngeal abscesses are deep neck space infections that can pose an immediate life-threatening emergency, with potential for airway compromise and other catastrophic complications [1]. The retropharyngeal space has a very complex anatomy, and is located posterior to the pharynx (naso-pharynx, oro-pharynx, and hypo-pharynx), larynx, and trachea. The anterior border of this space is formed by the bucco-pharyngeal fascia, which surrounds the pharynx, trachea, esophagus, and thyroid. The posterior boundary is formed by alar fascia; it is bounded laterally by the carotid sheaths and para-pharyngeal spaces. It extends superiorly to the base of the skull and inferiorly to the mediastinum at the level of the tracheal bifurcation. Para-pharyngeal space communicates with retropharyngeal space and thus an infection of retropharyngeal space can pass to the para-pharyngeal spaces as well as can go down in the mediastinum up to the tracheal bifurcation [2].
Retropharyngeal abscess is a disease of pediatric age group and majority of patients fall in this category, that may be because of prominent retropharyngeal group of lymph node in this age group and recurrent upper respiratory tract infections in children, the other common causes are trauma, foreign body impaction and immuno-compromised patients. Retropharyngeal abscess can lead to airway obstruction or sepsis - both life-threatening emergencies [3]. Fatalities normally occur from patients not receiving treatment immediately and suffocating prior to knowing that anything serious was wrong.
Material and Methods
This is a retrospective study of five cases with the discharge diagnosis of retropharyngeal abscess treated in the past 3 years. Only children below 12 years were taken in the study, a detailed analysis of the incidence pattern of the disease, age and sex analysis of the patients, the symptoms with which they presented, was analyzed. A thorough clinical examination of head and neck was done except endoscopy or direst laryngoscopy which was not done to avoid laryngospasm or accidental rupture of the abscess. Patients were subjected to radiological investigations and X-ray was done in all the cases and CT scan of neck could be done in 3 cases. Treatment modality used with outcome is presented in this study. Patients without confirmatory radiographic findings, fluoroscopy, or computed tomography (CT) were excluded.
Observations
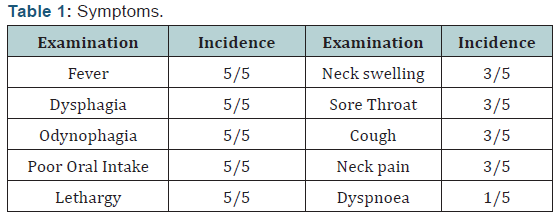
A total number of five cases have been taken in the present study treated in the past three years, The age group of the patients ranged from 3yrs to 10 yrs, (mean age was 5.2 yrs). Majority of the patients (60%) were males and from poor socioeconomic status. The chief complaints of the patients present in all the cases were (Table 1) Fever, Dysphagia, Odynophagia, Poor oral intake and lethargy which was present in 5/5=100% cases. Patients also complained of cough with sore throat and neck pain with neck swelling and stiffness (3/5=60%) Dyspnoea was present in (1/5=20%) cases.
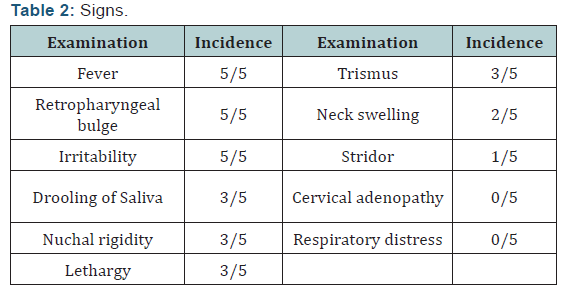
The findings on examination were (Table 2) - Irritability with fever and retropharyngeal bulge were found in all the patients (5/5=100%). 3/5 i.e. 60% patients had lethargy, nuchal rigidity and, drooling of saliva, trismus. Two patients (2/5=40%) has extension of the abscess in the neck presenting as neck swellings. Stridor was found in only one (1/5=20%) patient and no patient had respiratory distress or cervical adenopathy.
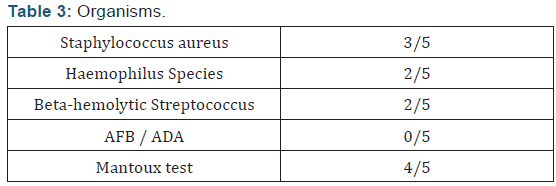
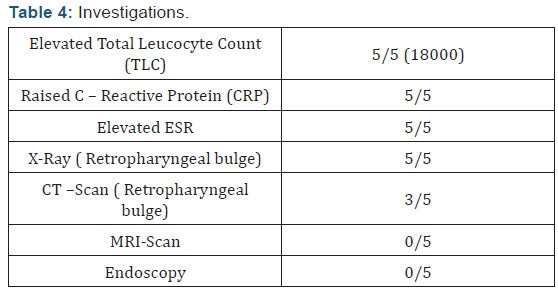
Culture of the pus removed showed mixed flora (Table 3) with staphylococcus aureus (3/5=60%), Haemophilus species (2/5=40%), Beta-hemolytic streptococcus (2/5=40%). All the specimens were negative for AFB staining, and ADA for tuberculosis was also normal in all the patients. Mantoux test was done in all the cases and was positive in 4/5=80% cases. Hematological profile reveled (Table 4) elevated total leukocyte count (with mean value being 18000), CRP and ESR in 5/5=100% cases. In radiological examination X-Ray was done in all the cases and showed retropharyngeal budge in 5/5=100% cases, only in one case (1/5=20%) there was an extension of the abscess in superior mediastinum. CT scan could be done only in 3/5=60% cases which showed retropharyngeal bulge in all the cases. None of the patient had any cervical lymphadenopathy, and neither CT scan nor X-ray showed any cervical vertebra anomaly. Endoscopic evaluation of Larynx was not done in any case because of the risk of trauma to abscess and chances of rupture.
All the patients were managed surgically under General anesthesia and aspiration technique was used (instead of giving incision in the lesion) in all the cases. Surprisingly the swelling in the neck (which was present in the neck in 2/5 patients) was also drained through the same aspiration site in the nasopharynx and no external incision was given to drain them. In the post operative period they were kept on IV antibiotics, in the NICU and ATT (four drug regimen) was started in 3/5=60% cases. In the earlier 2 cases when ATT was not given recurrence (refilling) of the retropharyngeal spaces was noticed and re-aspiration had to be done only once. None of the patients required Tracheostomy or postoperative ventilatory support.
Long term follow-up showed no significant residual disease or complications and ATT was given to all the three patients for a period of nine months.
Discussion
Retropharyngeal abscess is a rather rare, deep-neck infection of children and may seriously compromise the airway and mimic other diseases [4]. Abscesses in this space can be caused by many organisms such as aerobic organisms (beta-hemolytic Streptococci and Staphylococcus aureus), anaerobic organisms (species of Bacteroides and Veillonella), or Gram-negative organisms (Haemophilus parainfluenzae and Bartonella henselae) [5]. In our data were found a mixed infection of Staphylococcus aureu, Haemophilus species, and beta-hemolytic Streptococci.
The high mortality rate associated with retropharyngeal abscesses is due to its association with airway obstruction, mediastinitis, aspiration pneumonia, epidural abscess, jugular venous thrombosis, necrotizing fasciitis, sepsis, and erosion into the carotid artery [6], we did not encounter any of these in the present series. Retropharyngeal abscess is more common in males than in females [7] as was also the case in this study. The principal symptoms in adults are sore throat, fever, dysphagia, odynophagia, neck pain and dyspnoea. Patients with retropharyngeal abscesses may present signs of airway obstruction, but often they do not. The most common physical presentation is posterior pharyngeal edema (37%), nuchal rigidity, cervical adenopathy, drooling, and Stridor [8] which was also found in the present study except that cervical adenopathy was not found in any case.
CT contributes greatly to the diagnosis, but it has limitations in differentiating abscess from cellulites of the retropharyngeal space. The plain radiograph in lateral view is very specific when it shows air in the retropharyngeal space [7]. In our study both X-ray (5/5) and CT Scan (3/5) were equally helpful in the diagnosis. Cases of tubercular retropharyngeal abscess have been reported previously [9], and, in our series, we saw four cases of retropharyngeal abscess with positive Mantoux test, treated successfully with anti-Koch’s therapy. It was also observed that refilling of the aspirated retropharyngeal space was also reduced after anti-Koch’s treatment was started.
In nonspecific retropharyngeal abscess, antibiotic therapy (generally triple intravenous antibiotics: Co-amoxiclav, Amino glycoside, and Imidazole) alone may be insufficient, and most authors recommend combining it with a surgical drainage of the collection [10], which was done in all the cases in the present study. The ideal time to make the drainage is in dispute. Some suggest surgical drainage in cases of diabetes and tuberculosis and in other cases, the puncture of the abscess and the antibiotics are sufficient to control the collection and to obtain a favorable outcome [7]. In the present series although 4/5=80% cases had a positive Mantoux test , none had cervical vertebra anomaly and none were diabetic, hence only aspiration was done in all the cases and only in two cases refilling of the space was noticed and once respiration was done in both, interestingly in both these cases anti-Koch’s treatment was not given.
Conclusion
Retropharyngeal abscess are rare clinical conditions and can convert into a serious emergency if not treated properly, the present study concludes that:
- This condition is common in pediatric age group, and whenever patients present with Pain in throat, fever, cough, Odynophagia or Dysphagia, along with swelling in neck and sometimes respiratory distress, the diagnosis of Retropharyngeal abscess must be considered, as early diagnosis is the key to management and reducing morbidity and mortality.
- The diagnosis is based on the clinical and radiological pictures, which should be carried out as early as possible.
- It is very easy for a retropharyngeal abscess to spread to surrounding spaces especially Para pharyngeal spaces and into the mediastinum as all the neck spaces communicate with each other.
- The management of retropharyngeal abscess is based on antibiotics and surgical drainage/aspiration.
- Early drainage is the key to management as spontaneous rupture has catastrophic consequences.
- Adequate investigations to rule out tubercular etiology must be done and if found anti-Koch’s treatment must be started as soon as possible.
References
- Pediatric Retropharyngeal Abscess Author: Jason L Acevedo, MD; Chief Editor: Ravindhra G Elluru, MD, PhD
- John Grosso, Charles M Myer, Beverly P Wood (1990) Radiological Cases of the Month. Am J Dis Child 144(12): 1349-1350.
- McLeod C, Stanley KA (2008) Images in emergency medicine: retropharyngeal abscess. West J Emerg Med 9 (1): 55.
- Morrison JE, Pashley NR (1988) Retropharyngeal abscesses in children: A 10-year review. Pediatr Emerg Care 4(1): 9-11.
- Sato K, Izumi T, Toshima M, Nagai T, Muroi K, et al. (2005) Retropharyngeal abscess due to methicillin-resistant Staphylococcus aureus in a case of acute myeloid leukemia. Intern Med 44(4): 346-349.
- Herzon FS, Martin AD (2006) Medical and surgical treatment of peritonsillar, retropharyngeal, and parapharyngeal abscesses. Curr Infect Dis Rep 8(3): 196-202.
- A Harkani, R Hassani, T Ziad, L Aderdour, H Nouri, et al. (2011) Retropharyngeal Abscess in Adults: Five Case Reports and Review of the Literature. Scientific World Journal 11: 1623-1629.
- Pollard BA, El-Beheiry H (1999) Pott’s disease with unstable cervical spine, retropharyngeal cold abscess and progressive airway obstruction. Can J Anaesth 46(8): 772-775.
- Gunawardana SS, Earley AR, Pollard AJ, Bethell D (2004) Twelfth nerve palsy due to a retropharyngeal tuberculosis abscess. Arch Dis Child 89(6): 579.
- Wang LF, Kuo WR, Tsai SM, Huang KJ (2003) Characterizations of lifethreatening deep cervical space infections: a review of one hundred ninety-six cases. Am J Otolaryngol 24(2): 111-117.















