




Case Report
Three-Dimensional Identification of Eagle’s Syndrome- A Case Report
Hassan Baallal*, Akhaddar Ali, Gazzaz Miloud, el Moustarchid Brahim
Department of Neurosurgery, University of King Mohammed V Souissi, AfricaE
Submission: June 27, 2016; Published: July 11, 2016
*Corresponding author: Hassan Baallal, Department of Neurosurgery, University of King Mohammed V Souissi, Mohammed V Military Teaching Hospital, Rabat, Morocco, Africa, Tel: 212661295918; Email: baallalnch@gmail.com
How to cite this article: Hassan B, Akhaddar Ali, Gazzaz M, el Moustarchid B. Three-Dimensional Identification of Eagle’s Syndrome- A Case Report. Glob J Oto. 2016; 1(3): 555565. DOI: 10.19080/GJO.2016.01.555565
Abstract
The case in question is a 35-year-old man, with a For Peer Review history of bilateral laterocervical pain episodes radiating to the orbital region for over 3 years. He had no history of surgery or trauma. A careful clinical examination radiographs and 3D computed tomography scan revealed 47mm long bilateral styloid processes. In 1937 Eagle documented cases in which elongation of the styloid process (over 25 mm), appeared to be the cause of pharyngeal and cervical pain. Several pathophysiologic mechanisms leading to Eagle’s syndrome have been proposed, but all revolve around mechanical compression of the styloid processes on adjacent structures resulting in direct or referred pain.
Keywords: Elongated styloid process; Eagle’s syndrome
Introduction
Eagle syndrome is represented by alternate discomfort in the oropharynx that may emit to the labyrinth; zygomatic bone; or nape it is generally characterized as dul and persistent another ordinary manifestations include pain with rotation of the head [1-4]; dysphagia; trigeminal neuralgia. It is rarely announced [4,5]. Eagle syndrome is provoked by a prolongation styloid, process that compresses nearby formations including, nerves and blood vessels, usual styloid processes are, intermediate to 2.5 and 3.0cm in length. Linear distance greater than 3cm are treated elongated [5,6].
Case Report
The case in question is a 35-year-old man, with a For Peer Review history of bilateral laterocervical pain episodes radiating to the orbital region for over 3 years. He had no history of surgery or trauma. He was presented with trigeminal neuralgia at the commencement of the functional disorder and was treated unsuccessfully with carbamazepine since then Physical examination mentioned intensification of the pain by palpation of the tonsillar fossa. Cervical Computed tomography with three-dimensional reconstruction reveal elongation of the styloid processes that were 47mm long on the two sides (Figure 1). The findings were compatible with Eagle syndrome and the patient established of symptomatic treatment, prosthetic rehabilitation and succeeding clinical follow up without have use for any surgery.
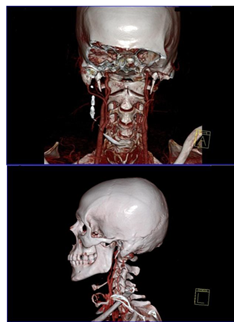
Figure 1: Three-dimensional identification of eagle’s syndrome using computed tomography.
Discussion
Styloid process (SP) is a cylindrical structure in front of the stylomastoid foramen, inferior and anterior, extending from the inferior face of the petrous part of the temporal bone toward the tonsillar fossa between the internal and external carotid arteries. The SP proceeds as the stylohyoid ligament and attaches to the lesser horn of the hyoid bone. The internal jugular vein, vagus, glossopharyngeal, accessories, and hypoglossal nerve, internal carotid artery, sympathetic chain, and sphenomandibular ligament are located at its medial point [7-12]. Stylohyoid complex develops from the second branchial (Reichter cartilage) arch. Stylohyoid complex consists of four segments: [8-10].
In1937, Eagle reported two observations in which an elongated styloid process had relations with facial spasm more uncommonly, symptoms such as dysphagia, and/or facial pain recurrent throat pain, foreign body sensation, as a direct result of an elongated styloid process or calcified stylohyoid ligament [13]. However that may be proximately 4% of the population is thought to have an elongated styloid process, just among 4% and 10.3% of this category is thought to truly be symptomatic [14]. The authentic etiology of the elongated SP due to calcified and ossified bone and ligament is not explicit. It was proposed that endocrine disorders in female at menopause, persistence of mesenchymal elements, surgical trauma; local chronic irritations, growth of the osseous tissue and mechanical stress or trauma during development of SP could result in calcified hyperplasia of the SP [15,16]. Eagle syndrome is now thought to be due to 2 distinct variety, the standard form succeeding from cranial nerve intrusion causing stretching of the XII cranial nerve [17-20] and the second type from distraction of the carotid vessels.
In a research, Okabe et al. [21] discovered a notable relationship between the serum calcium (Ca) concentration and the SP length among 80-year-old subjects. The longer the SP was, the higher the serum Ca concentration was in this sample. They also evaluated the correlation between the SP length and heel bone density in these subjects. Management is medical or surgical but there is a lack of evidence, particularly on non-surgical options. These include; nonsteroidal anti inflammatory drugs, diazepam, carbamazepine, heat application, transpharyngeal injection of local analgesia, and physiotherapy. Surgery is by the transphayrngeal or extra-oral approach and may be curative. The extra-oral approach involves external scarring, but provides better visualisation of the surgical field and reduced risk of infection. But the less invasive transpharyngeal route may predispose to injury of local structures, infection, and post-procedure oedema, due to a limited surgical field. While surgical failure rates of around 20% have been described, more recent studies demonstrate complete resolution of symptoms in most cases with few post-operative complications, chiefly a transient marginal mandibular nerve weakness [22].
Conclusion
Eagle syndrome is a unusual pathology, whichever be diagnosed by associating physical examination and radiographic examinations together. Its treatment success is determined by constituting a exact diagnosis and taking into account the symptoms to select between a medical or surgical treatment. In this particular case, the symptomatic treatment was realized, prosthetic rehabilitation and subsequent clinical follow up without the need of any surgical intervention.
References
- Slavin KV (2002) Eagle syndrome: entrapment of the glossopharyngeal nerve Case report and review of the literature. J Neurosurg 97(1): 216- 218.
- Ceylan A, Köybaşioğlu A, Celenk F, Yilmaz O, Uslu S (2008) Surgical treatment of elongated styloid process: experience of 61 cases. Skull Base 18(5): 289-295.
- Sun CK, Mercuri V, Cook MJ (2006) Eagle syndrome: an unusual cause of head and neck pain. Arch Neurol 63(2): 294 -295.
- Strauss M, Zohar Y, Laurian N (1985) Elongated styloid process syndrome: intraoral versus external approach for styloid surgery. Laryngoscope 95(8): 976-979.
- Mortellaro C, Biancucci P, Picciolo G, Vercellino V (2002) Eagle’s syndrome: importance of a corrected diagnosis and adequate surgical treatment. J Craniofac Surg 13(6): 755-758.
- Koivumäki A, Marinescu-Gava M, Järnstedt J, Sándor GK, Wolff J (2012) Trauma induced eagle syndrome. Int J Oral Maxillofac Surg 41(3): 350- 353.
- Palesy P, Murray GM, De Boever J, Klineberg I (2000) The involvement of the styloid process in head and neck pain a preliminary study. J Oral Rehabil 27(4): 275-287.
- 8. Ateşçi M, Karabacakoglu A, Gülmez U (2010) Left internal carotid compression due to deviation of elongated styloid process: case report. Turkiye Klinikleri J Cardiovasc Sci 22(1): 140-143.
- Balcioglu HA, Kilic C, Akyol M, Ozan H, Kokten G (2009) Length of the styloid process and anatomical implications for Eagle’s syndrome. Folia Morphol (Warsz) 68(4): 265-270.
- Başekim CC, Mutlu H, Güngör A, Silit E, Pekkafali Z, et al. (2005) Evaluation of styloid process by three-dimensional computed tomography. Eur Radiol 15(1): 134-139.
- Ghosh LM, Dubey SP (1999) The syndrome of elongated styloid process. Auris Nasus Larynx 26(2): 169-175.
- Balbuena L, Hayes D, Ramirez SG, Johnson R (1997) Eagle’s syndrome (elongated styloid process). South Med J 90(3): 331-334.
- Rechtweg JS, Wax MK (1998) Eagle’s syndrome: a review. Am J Otolaryngol 19(5): 316-321.
- Krennmair G, Piehslinger E (2003) Variants of ossification in the stylohyoid chain. Cranio 21(1): 31-37.
- Prasad KC, Kamath MP, Reddy KJ, Raju K, Agarwal S (2002) Elongated styloid process (Eagle’s syndrome): a clinical study. J Oral Maxillofac Surg 60(2): 171-175.
- Monsour PA, Young WG (1986) Variability of the styloid process and stylohyoid ligament in panoramic radiographs. Oral Surg Oral Med Oral Pathol 61(5): 522-526.
- Moffat DA, Ramsden RT, Shaw HJ (1977) The styloid process syndrome: aetiological factors and surgical management. J Laryngol Otol 91(4): 279-294.
- Lindeman P (1985) The elongated styloid process as a cause of throat discomfort. Four case reports. J Laryngol Otol 99(5): 505-508.
- Boddour HM, McAnear JT, Tilson HB (1978) Eagle’s syndrome. Report of a case. Oral Surg Oral Med Oral Pathol 46(4): 486-494.
- Ceylan A, Köybaşioğlu A, Celenk F, Yilmaz O, Uslu S (2008) Surgical treatment of elongated styloid process: experience of 61 cases. Skull Base 18(5): 289-295.
- Okabe S, Morimoto Y, Ansai T, Yamada K, Tanaka T, et al. (2006) Clinical significance and variation of the advanced calcified stylohyoid complex detected by panoramic radiographs among 80-year-old subjects. Dentomaxillofac Radiol 35(3): 191-199.
- Ceylan A, Köybaşioğlu A, Celenk F, Yilmaz O, Uslu S (2008) Surgical treatment of elongated styloid process: experience of 61 cases. Skull Base 18(5): 289-295.















