



The Extension Block Technique for the Treatment of Mallet Finger Fracture
Ricardo Monreal*
Clínicas Maison de Santé, South America
Submission: October 29, 2016; Published: November 03, 2016
*Corresponding author: Ricardo Monreal, Clínicas Maison de Santé, Ave. Chorrillos 171, Chorrillos, Lima, Peru, Email:rmonreal59@yahoo.es
How to cite this article: Ricardo M. The Extension Block Technique for the Treatment of Mallet Finger Fracture. Ortho & Rheum Open Access J. 2016; 3(3): 555615. DOI: 10.19080/OROAJ.2016.03.555615
Introduction
The management of intra-articular fractures of the hand represents a challenge. Large articular fragments require reduction and operative fixation. A number of surgical techniques have been described in literature, with variable results. Distal interphalangeal joint fractures have been fixed by various methods including screw, plate and suture techniques. Generally operative fixation is indicated when more than 30% of the articular surface is involved with or without subluxation of the joint. The aim of surgery is to reduce the fracture fragments anatomically whilst providing osseous stability, and to commence early active movement of the joint to prevent stiffness. The treatment options for mallet fractures of the distal phalanx range from splinting [1], to surgical fixation using percutaneous pins [2,3], pull-out wires [4], microscrews [5] or interosseous wires [6].
While conservative treatment with splints is successful in most cases, surgery should be considered when one third or more of the articular surface of the distal phalanx is involved. This paper describes the results obtained using a minimal invasive technique (extension block K-wire fixation technique) which was first described by Ishiguro et al. [7] and Darder-Pratset [8]. The indications for this technique include the presence of a large bone fragment, palmar subluxation or loss of joint congruity of the distal interphalangeal joint or an extension lag of more than 30°.
Abbreviations
DIPJ: Distal Interphalangeal Joint; PIPJ: Proximal Interphalangeal Joint; MPJ: Metacarpophalangeal Joint
Patients and Methods
The study group comprised 10 patients (10 fingers) with a bony mallet finger deformity treated by the extension block technique between 2011 and 2013. Patients included 9 males and 1 female with a mean age of 27 years (range, 16-44 years). The long finger was the most commonly affected (4 cases), followed by the ring finger (3 cases), index finger (2 cases), and little finger (1 case). The inclusion criteria were:
- a dorsal intra-articular fracture fragment involving >30% of the base of the distal phalanx with or without volar subluxation of the distal phalanx,
- patients where fracture reduction was not proper after application of mallet finger splint,
- no limitation in passive motion of the distal interphalangeal and proximal interphalangeal joints and no swan-neck deformity; and
- <6 weeks delay from the injury without treatment. Patients with comminuted or open fractures were excluded. Informed consent was obtained from all patients [verbal and written]. Digit are obtained to determine comminution, subluxation of the joint and to determine the articular fragment size. Mallet fractures are classified by the Wehbe & Schneider [9] method based on the degree of subluxation of the distal phalanx and the size and displacement of the fracture fragment (Table 1).
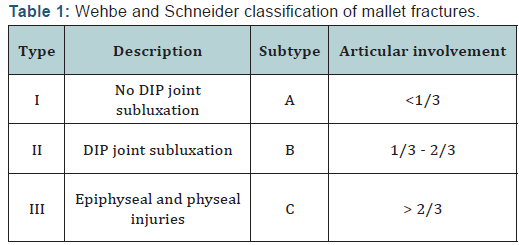
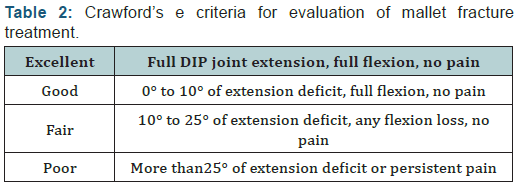
According to Wehbe´ & Schneider’s [9] classification, there were 6 type IB, and 4 type IIB injuries. Themean time from the injury to surgery was 16 days (range, 3-22 days). Patients were evaluated clinically and radiologically. Clinical results were assessed using the criteria published by Crawford [1] (Table 2). Radiographs were taken of all cases after surgery. On radiographs were evaluated: union, malunion, space, inclination, degenerative changes, subluxation and deformity.
Surgical technique
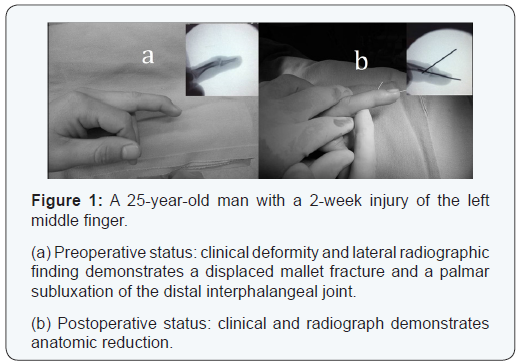
The operation is performed under digital block anesthesia. Distal interphalangeal joint (DIPJ) is passively flexed so that the displaced fragment moves to its original position because of to maintain continuity periosteal. A 0.035” [0.9 mm] or 0.045” (1.4 mm) K wire is inserted through the extensor tendon at a 45 degree angle into the head of the middle phalanx along the dorsal edge of the fragment under the surveillance of C-arm. The distal phalanx is extended to 0°. A second K wire is inserted to transfix the DIPJ in to the middle phalanx to maintain reduction. Fluoroscopic verification of fracture reduction and wire position should be obtained in all patients (Figures 1 & 2). The wires are cut short and regular dressing and pin care hygiene is encouraged. Active motion of the proximal interphalangeal joint (PIPJ) and metacarpophalangeal joint (MPJ) started immediately after the surgery. Splinting was not used. The follow up visit was conducted ten days after the surgery to evaluate the site of the pin. The K wires are removed 6 weeks postoperatively when the bridging trabeculae are observed on radiographs and full active and passive exercises are then initiated and daily activities were not restricted.
Results
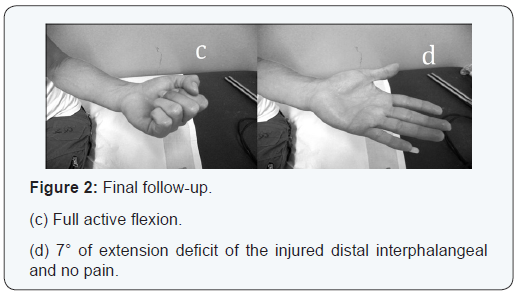
Radiographic bone union was achieved in all patients in a mean of 6.5 weeks (range, 6-7.3 weeks). The mean extensor lag of the distal interphalangeal joint was 22° (range, 10°- 38°) preoperatively, which was improved to 5° (range, 0°-8°) postoperatively. The mean flexion of the distal interphalangeal joint was 78° (range, 71°-90°). Using the Crawford’s evaluation criteria, 3 patients (3 fingers; 30%) had excellent results, 6 (60%) had good results (Figure 2), and 1 (10%) had fair result. There were no poor results. None of these patients at final follow-up required further treatment.
Discussion
Mallet fractures involve avulsion of the dorsal base of the distal phalanx with the attached extensor tendon. Disruption of the extensor mechanism results in a characteristic flexion deformity of the DIPJan axial load which forcibly flexes an extended finger and commonly results from ball related sporting activities [10]. Larger mallet fractures can be a result of hyperextension and impaction forces [11]. An accompanying hyperextension of the proximal interphalangeal joint or swanneck deformity is possible in each type. The management of mallet fractures, whether conservative or operative, has remained controversial as no single treatment modality has shown to resolve issues with arthritis, deformity, stiffness and complications [6,12]. Suboptimal treatment can lead to extensor lag, swan neck deformity and post traumatic osteoarthritis [9,13]. Mallet avulsion fractures are most often treated in a closed manner when there is less than one third of the articular surface involved with no volar subluxation, then DIPJ extension splinting for 6 to 8 weeks can be used, followed by gradual introduction of active flexion.
The ideal treatment for a mallet finger fracture which involves more than one third of the articular surface remains controversial. Operative fixation has been advocated when the mallet avulsion fracture involves a fragment greater than one third (>30%) of the articular surface, or in case of persistent volar subluxation and displacement of the fracture fragment despite splintage of the DIPJ in full extension [12]. Some authors have advocated that the operative goal is to maintain a stable arc of motion of the DIPJ without subluxation [14] whilst others have advocated anatomical reduction and internal fixation to prevent residual deformity, post traumatic arthritis and stiffness [15].
We have found that the extension block technique previously described by Ishiguro et al. [7] and Darder-Pratset [8] is effective and minimally invasive, and it does not disrupt the remaining extensor mechanism. It is also a relatively easy to achieve an adequate reduction and good fixation under image. Furthermore, it allows an earlier mobilization of the involved joint [as soon as the pins are removed], making it a more suitable procedure for patients who require early use of the hand. This procedure is best used in acute injuries, but can also be used for cases, which present up to 5 weeks after injury, although the presence of a fracture which is more than 8 weeks old is a contraindication.
For fractures older than 2 weeks, Ishiguro [7] recommended using the tip of an injection needle (18 g needle) to freshen the fracture surfaces before using the extension block pinning technique. This technique provides the stability of surgical fixation without relying on surgical exposure or splints, thereby eliminating the associated risks with these treatments. In contrast, treatment is more controversial when the fragment involves more than one-third of the articular surface, and many treatment modalities have been suggested as the best fixation technique for a mallet fracture [1-5,16]. Potential disadvantages include articular cartilage damage leading to secondary osteoarthritis, especially if more than one attempt at pin insertion is needed.
Conclusion
Although the present paper is a retrospective review of a single surgeon’s experience, we conclude that the extensionblock K-wires fixation technique provides an alternative and acceptable treatment modality for the treatment of bony mallet finger deformities with or without subluxation of the distal phalanx.
Statement of Informed Consent
All study participants provided informed written consent prior to study enrollment.
Statement of Human Rights
All procedures followed were in accordance with the Helsinki Declaration of 1975, as revised in 2008. Informed consent was obtained from all patients for being included in the study.
References
- Crawford GP (1984) The molded polythene splint for the mallet finger deformities. J Hand Surg Am 9(2): 231-237.
- Badia A, Riano F (2004) A Simple Fixation Method for Unstable Bony Mallet Finger. J Hand Surg Am 29(6): 1051-1055.
- Kondo M, Minami M, Kato S, Minami A, Kaneda K (1998) New method in the treatment of mallet fracture. Tech Hand Up Extrem Surg 2(3): 206-209.
- Damron TA, Engber WD (1994) Surgical treatment of mallet finger fractures by tension band technique. Clin Orthop Relat Res 300: 133- 140.
- Sakaue M, Sumimoto Y, Omori K, Yoshida M (1986) Treatment of mallet finger using a micro screw. Journal Japanese Society Surgery Hand 3: 538-541.
- Jupiter JB, Sheppard JE (1987) Tension wire fixation of avulsion fractures in the hand. Clin Orthop Relat Res 214: 113-120.
- Ishiguro T, Itoh Y, Yabe Y, Hashizume N (1997) Extension block with Kirschner wire for fracture dislocation of the distal interphalangeal joint. Tech Hand Up Extrem Surg 1(2): 95- 102.
- Darder-Prats A, Fernandez-Garcia E, Fernandez-Gabarda R, Darder- Garcia A (1998) Treatment of mallet finger fractures by the extensionblock K-wire technique. J Hand Surg Br 23(6): 802-805.
- Wehbe´ MA, Schneider LH (1984). Mallet fractures. J Bone Joint Surg Am 66(5): 658-669.
- McCue FC 3rd, Meister K (1993) Common sports hand injuries. An overview of aetiology, management and prevention. Sports Med 15(4): 281-289.
- Lange RH, Engber WD (1983) Hyperextension mallet finger. Orthopedics 6(11): 1462-1421.
- Damron TA, Engber WD, Lange RH, McCabe R, Damron LA, et al. (1993) Biomechanical analysis of mallet finger fracture fixation techniques. J Hand Surg Am 18(4): 600-608.
- Garberman SF, Diao E, Peimer CA (1994) Mallet finger: results of early versus delayed closed treatment. J Hand Surg Am 19(5): 850-852.
- Niechajev IA (1985) Conservative and operative treatment of mallet finger. Plast Reconstr Surg 76(4): 580-585.
- Hamas RS, Horrell ED, Pierret GP (1978) Treatment of mallet finger due to intra-articular fracture of the distal phalanx. J Hand Surg Am 3(4): 361-363.
- Kang HJ, Shin SJ, Kang ES (2001) Complications of operative treatment for mallet fractures of the distal phalanx. J Hand Surg Br 26(1): 28-31.















