



Fibrolipomatous Hamartoma of Median Nerve: An MRI Diagnosis
*Naveen Rajadurai
Hospital Sungai Buloh, Ministry of Health, Malaysia
Submission: October 21, 2016; Published: November 02, 2016
*Corresponding author: Naveen Rajadurai, 151-6-8, Menara Duta Condo, Jalan Dutamas Raya, 51200 Kuala Lumpur, Malaysia, Tel:60122728630 ; Email: drnavraj@yahoo.com
How to cite this article: Naveen R. Fibrolipomatous Hamartoma of Median Nerve: An MRI Diagnosis. Ortho & Rheum Open Access J. 2016; 3(3): 555614. DOI: 10.19080/OROAJ.2016.03.555614
Abstract
Fibrolipomat ous hamartoma is a rare benign tumour affecting pre dominantly the median nerve. Pathognomonic MRI features of coaxial cable-like appearance on axial images or spaghetti shaped enlarged nerve fascicles and fibrous tissue should point to a definitive diagnosis. Unnecessary biopsy can be avoided. The likelihood of the tumour growth to follow a branching pattern of the nerve and variation in distribution of mature fat within the lesion are additional features pointing towards the diagnosis of this entity.
Introduction
Fibrolipomatous hamartoma is a rare condition with characteristic MRI findings that affects the median nerve which may obviate unnecessary biopsy. The tumour consists of perineural and endoneural fibrosis causing thickening of the neural fascicles. Treatment depends on the extent of nerve involvement as catastrophic motor and sensory deficit have been reported following complete resection. We report a case of fibrolipomatous hamartoma in a gentleman who was symptomatic and was initially diagnosed purely by the imaging features. He was successfully operated and histopathology specimen confirmed the diagnosis. He was discharged well and follow up showed no recurrence.
Case Report
A 34-year-old Nepali man presented to our hospital a year ago with a rapidly enlarging lesion in the right palm, over a period of 5 months. This lesion had been present for the past 10 years, but initially measured 1cm in size. It had increased to its current size of 6cm diameter over 5 months. No neurological deficit, pain or signs of inflammation were present. On physical examination, there was a non-tender swelling on the thenar aspect of the right palm with reduced grip strength but intact sensation. Plain radiographs showed a soft tissue bulge without calcification between the 1st and 2nd metacarpal. There was no periosteal reaction or bone remodeling. MRI findings revealed an elongated mass along the segment of median nerve in the carpal tunnel which had extended to involve the 1st digital branch of the median nerve (Figure 1).
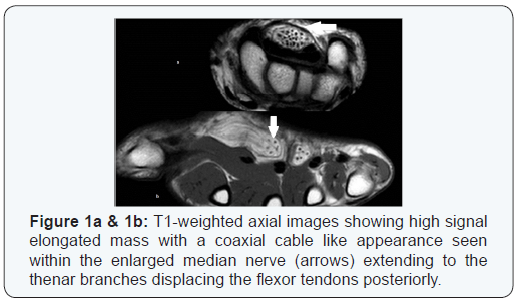
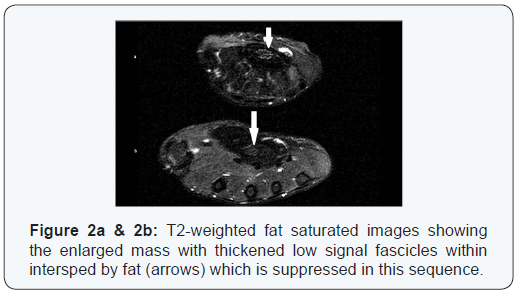
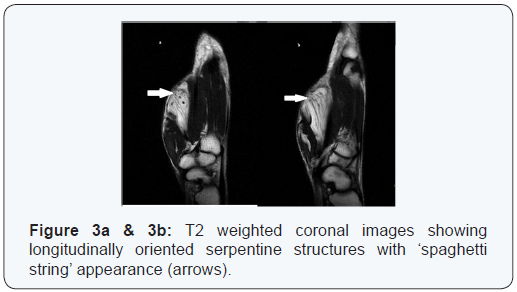
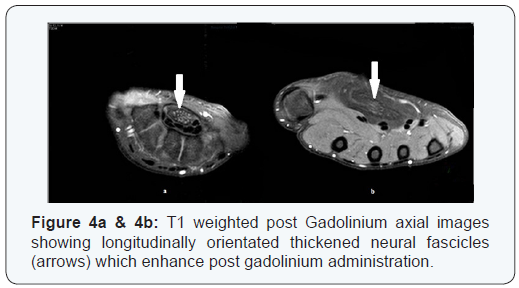
The tendons in carpal tunnel region were displaced posteriorly with no underlying bony erosion, marrow infiltration or vessel anomaly demonstrated. The mass comprised of longitudinally oriented serpentine structures that demonstrated low signals in both T1W and T2W images. These serpentine structures enhanced with intravenous gadolinium, suggestive of thickened neural fascicles with endoneural and perineural fibrosis. The fascicles were interspersed by fatty tissues which appeared more abundant distally (Figure 2). On axial images, the tumour had coaxial cable-like appearance while on coronal images it had a “spaghetti string” appearance (Figure 3). This constellation of findings is pathognomonic of fibrolipomatous hamartoma.
At surgery, the median nerve was found to be enlarged and tortuous from the level of the carpal tunnel and extending distally. The nerve was enveloped with fibrous tissue and fat. The branches to the thenar muscles and 1st digital branch of the median nerve was also infiltrated by the tumour and were thickened. The carpal tunnel was opened and excision of the lesion was performed. Grossly the tumour appeared pink and yellow in colour. Histopathological examination confirmed diagnosis of fibrolipomatous hamartoma with mature benign fibro-fatty soft tissue. No post operative neurological deficit was seen (Figure 4).
Discussion
Fibrolipomatous hamartomas are benign tumors usually affecting infants and less commonly children and young adults [1]. Of all tumours in the upper extremity, 2% are nerve tumours [2]. Schwannoma is probably the most frequent one with a known incidence of less than 1/100000 inhabitants a year in Sweden [3]. Usually, the diagnosis of a nerve tumour has to be based on microscopical findings since MRI is not sufficient for a precise diagnosis [4]. In contrast, fibrolipomatous hamartoma, which is even rarer, has very distinct characteristics in MRI. On reviewing the literature there are only approximately 92 cases of this entity that have been reported.
These tumours have come to be known as fibrolipomatous nerve sheath enlargement, perineural and intraneurallipoma, lipofibromatous hamartoma, lipofibroma, fibro-fatty overgrowth, fatty infiltration of nerve, fibro-fatty nerve enlargement, and fatty infiltration of the median nerve [5,6]. More than 80% of these tumours affect exclusively the median nerve. Other sites affected rarely are the ulnar nerve, radial nerve, axillary nerve, musculocutaneous nerve, brachial nerves, cranial nerves and lower limb nerves which range from 4-22% [7]. In 20-67%, this condition can be associated with macrodystrophialipomatosa which affects the 2nd and 3rd digits [8]. Fibrolipomatoushamartoma patients usually present in the 3rd to 4th decades of life with a long history of a soft, slowly enlarging painless mass since childhood. Late signs and symptoms are associated with nerve compression in the distribution of the affected nerve and patients present with pain, paresthesia and motor deficit.
On histological correlation, perineural and endoneural fibrosis cause thickening of the neural fascicles with mature fatty infiltration of the interfascicular connective tissue [8]. The perineural and endoneural fibrosis accounts for the lowsignal intensity of the thickened nerve fascicles which appear as serpentine structures longitudinally oriented along the nerve on MRI. On axial images, the enlarged nerve bundles, with its thickened nerve fascicles interspersed with infiltrating fat, have a coaxial cable-like feature which is pathognomonic of fibrolipomatous hamartoma. Apart from the segment of median nerve in the carpal tunnel, the 1st digital branch and branches to the thenar muscles were also involved in this patient.
The differential diagnosis of this tumour includes intraneurallipoma, ganglion cyst, traumatic neuroma, schwannoma, tenosynovitis and vascular malformation in which the signal void areas can mimic serpentine low-signal fibrotic neural fascicles. The presence of mature fat within this lesion excludes all other differentials except intraneurallipoma. In the case of intraneurallipoma, the fat content arises from the fatty tissue within the epineurium, presenting as a mass separate from the neural fascicles, instead of infiltrating in between and separating the neural fascicles as in fibrolipomatous hamartoma. Sonography of fibrolipomatous hamartoma also shows characteristic hypoechoic coaxial cabling, which corresponds to the thickened fibrotic neural fascicles encased by echogenic fatty substratum.
Sonography may be a more convenient and easily available diagnostic tool. Plain X-rays for patients without macrodystrophicalipomatosa are usually of normal appearance or show only a soft-tissue mass. When there is macrodystrophicalipomatosa, characteristic osseous and soft tissue changes are obvious. Management is usually conservative. When the patient is symptomatic indicating a severe compression element, decompression surgery as of the carpal tunnel in this patient with median nerve involvement has been shown to provide adequate relief of symptoms.
Conclusion
Fibrolipomatous hamartoma is a rare benign tumour affecting predominantly the median nerve. Pathognomonic MRI features of coaxial cable-like appearance on axial images or spaghetti shaped enlarged nerve fascicles and fibrous tissue should point to a definitive diagnosis [5,6]. Unnecessary biopsy can be avoided. The likelihood of the tumour growth to follow a branching pattern of the nerve and variation in distribution of mature fat within the lesion are additional features pointing towards the diagnosis of this entity.
References
- Anthony G Gilet, Jeremy M Baum, Elaine S Gould (2008) Fibrolipomatous Hamartoma of the Median Nerve. Radiology Case Reports 3(3): 195.
- Adani R, Baccarani A, Guidi E, Tarallo L (2008) Schwannomas of the upper extremity: diagnosis and treatment. Chir Organi Mov 92(2): 85- 88.
- Sandberg K, Nilsson J, Soe Nielsen N, Dahlin LB (2009) Tumours of peripheral nerves in the upper extremity: a 22-year epidemiological study. Scand J Plast Reconstr Surg Hand Surg 43(1): 43-49.
- Nilsson J, Sandberg K, Nielsen NS, Dahlin LB (2009) Magnetic resonance imaging of peripheral nerve tumours in the upper extremity. Scand J Plast Reconstr Surg Hand Surg 43(3): 153-159.
- Cavallaro MC, Taylor JA, Gorman JD, Haghighi P, Resnick D (1993) Imaging Findings in a Patient with Fibrolipomatous Hamartoma of the Median nerve. AJR Am J Roentgenol 161(4): 837-838.
- De Maeseneer M, Jaovisidha S, Lenchik L, Witte D, Schweitzer ME, et al. (1997) Fibrolipomatous hamartoma: MR imaging findings. Skeletal Radiol 26(3): 155-160.
- Murphey MD, Smith WS, Smith SE, Kransdorf MJ, Temple HT (1999) From the Archives of the AFIP: Imaging of Musculoskeletal Neurogenic Tumors: Radiologic-Pathologic Correlation. Radiographics 19(5): 1253-1280.
- Silverman TA, Enzinger FM (1985) Fibrolipomatous hamartoma of nerve: A clinicopathologic analysis of 26 cases. Am J Surg Pathol 9(1): 7-14.















