




Pressure Plate Fixation according to Brunner & Weber for the Treatment of Recalcitrant Non-Union of the Femur. A Theoretical -Biomechanical Analysis
Reynders Frederix Pieter1*, Reynders Frederix Cristina2 and Illes Tamas1
1Department of Orthopedics & Traumatology, University Hospitals Brussels, Belgium
2Department of Medical Rehabilitation, University Hospitals Brussels, Belgium
Submission: May 10, 2017; Published: June 06, 2017
*Corresponding author: Reynders Frederix Pieter, Department of Orthopedics & Traumatology, University Hospitals Brussels, Brussels 1020m, Belgium; Tel: 32473361420; Email: reynders52@hotmail.com
How to cite this article: Reynders F P, Reynders F C Illes T. Pressure Plate Fixation according to Brunner & Weber for the Treatment of Recalcitrant Non-Union of the Femur. A Theoretical -Biomechanical Analysis. Nov Tech Arthritis Bone Res. 2017; 1(2) : 555559. 006 DOI: 10.19080/NTAB.2017.01.555559
Abstract
Objectives: Investigate experimentally the biomechanical advantages of the "wave”plate described by Weber & Brunner.
Structure:
1. Theoretical analysis of the neutral axis and stress distribution through the bone-plate composite beam in comparison with a normal femur plate.
2. Intraoperative monitoring of the pressure inside a non-union using a prescale pressure sensitive film: without a plate, with a plate, with a "wave” plate and with a "wave” plate in combination with an autologous iliac strut graft underneath the trapezoidal curve of the plate.
3. Mechanical testing of different plate fixations modes on a plastic femur model. Comparison was made between a regular conventional femur plate, a locked compression plate LCP and there Wave variants with or without a solid plastic bone block underneath the wave of the plate.
Results: The theoretical analysis shows that the neutral axis of "wave” plate-bone composite beam shifts outside the bone and all the compressive forces are acting through the cis and transcortex at the non-union site so less stress is transmitted through the plate. With the intra-operative measurements of the bending moment in two patients we observed stress shielding of the momentum in the frontal plane, when an iliac strut graft was pressed to the lateral site of the non-union beneath the curved portion of the plate.
With the mechanical testing of different plate designs with and without a solid plastic block underneath the wave of the plate we found a high pressure contact area in between the two main femur fragments with the wave plate. Mechanically we found no advantage of a wave plate in LCP version than with the wave plate made from a conventional femur plate. Adding a bone block underneath the wave of the plate possibly opens the fracture side asymmetrically by the three point fixation of the bone block pressing on the lateral surface of the femur. This bone block alters the force distribution around the fracture side.
Keywords: Fractures; Complication of fractures; Femoral fractures
Introduction
Most femoral fractures heal well with appropriate treatment. Failure of a fracture to heal is often multifactorial [14]. Fractures in the metaphyseal-diaphyseal transition zone that are provoked by the dissipation of high energy are notorious for their complications; such as infections, non-union, mal- union [5-9]. Delayed union implies slow healing, longer than is reasonably expected for a given fracture. Non-union occurs when a fracture has ceased to show any evidence of healing, as indicated by persistent fracture lines, sclerosis at the fragment ends and hypertrophic or absent callus. ‘Wave’ plate fixation is a form of bridging plate fixation which also tries to enhance the ‘tension band'effect by increasing the offset of an appropriately contoured plate from the loading axis of the femur [2,10].
In a previous study the authors reported promising results [11] on eight cases of long standing (more than three years) non-union of the femur treated with the compression "wave " plate according to Weber [12] and Brunner [13]. In this study we try to substantiate the alleged benefit of using an autologous iliac strut graft beneath the contoured segment of the plate in decreasing the load on the plate.
Material & Methods
Intra-operative measurements with pressure sensitive film (fuji prescale film: mitsui & co, los angeles, USA, ppf )
After obtaining the patient's consent and agreement of the local ethical committee, we could perform in one case in vivo measurement of pressure distribution at the non-union site in a 24 years-old male scheduled for a surgical revision of his proximal femoral non-union. The patient was victim of a road traffic accident six months ago, causing an open Gustilo Ilia communitive proximal femur fracture (Figure 1).



A single sheet Fuji Prescale Film was used to record the pressure inside the non-union area and beneath the plate (Figure 2a & 2b). With single sheet LLW Prescale film (0.5-2.5Mpa, 1Mpa=10, 2kgf/cm2), the colour forming layer is coated on the polyester base film. Micro encapsulated colour forming material is layered on the top of the film. When pressure is applied on the film, the microcapsules are broken with distribution and "density” of magenta colour depending on true pressure distribution and magnitude.
The PPF film was cut to the required size and mounted into a sterile protection sheet Figure 3 and placed between the two distracted main fragments of the femur after which distracting was released Figure 4.



Six settings were considered; pressure inside the non-union without plate fixation, with a conventional plate and a "wave" plate with and without an iliac strut graft pressed beneath the contoured bend of the plate. Finally through a 6mm thick Schanz screw, introduced medio-lateral in the femoral condyle, a bending moment of 100N and 300N in the frontal plane was applied with a dynamometer (Pesola AG, Rebmatti 19,CH-6340 Baar, Switzerland) (Figure 5).
The length of the lever arm between the centre of the femoral condyles and the attachment of the dynamometer is 10cm creating a bending moment of 100Nm and 300Nm. The PPF film was introduced into the biological inactive non-union after cleaning the non-union gap of fibrous tissue. The fracture surfaces were made as smooth as possible. Distraction the fracture was done using the pelvic clamp of Jungbluth. Every mechanical situation was recorded one time. Impressed results were measured by visual inspection toward a standard reference sample table and with an electronic densitometer (FPD-305E, FPD-306E). Prescale Sensitive Pressure Films) (Figure 6).

Theoretical mechanical analysis of conventional - and wave plate osteosynthesis

A fractured and stabilized femur was modeled. The femur is a hollo w cylinder with an external radius R=20mm and M=80Nm. The fracture is flat and spans the whole section of the bone. The remaining cortical bone has a stiffness of 18Gpa and has not deteriorated by the fracture. Stresses in bone and plate were calculated in five situations, depending on the amount of bone capable of load-bearing (grey zones in Figure 7):
a. The whole section.
b. All but the medial cortex.
c. Half of the section.
d. Only the lateral cortex.
e. Only the plate.
The fixation plate is modeled as a stainless steel plate (E=210Gpa) with rectangular cross section (h=6.4 mm, b=17mm) which is rigidly fixed to the bone. Three fixation modes were considered: d=0mm for a conventional (good contact between the plate and the lateral cortex) and d=5 (five mm offset between the plate and lateral cortex) and 10mm (ten mm offset between the plate and the lateral cortex) for a "wave" plates fixation.
The position of the neutral line (medial to this line are recorded compression forces and lateral to this line the bone is subjected to tension forces) is calculated from the following equation:
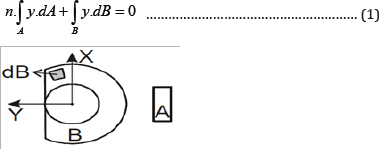
A = cross sectional area of the plate.
B = cross sectional area of the loaded bone.
n = Eplate/Ebone
y = the postion on the y axis of an elementary surface.
Y_max & y_min the outermost position of the bone on the medial and lateral end in relation to the neutral line.
The results for yn is shown in the graphic (Figure 7) for the three different types of plate (d=0, d=5mm, d=10mm) and weight bearing area of the bone (shaded area is the loaded area of the bone section). From these graphics one can discern that the neutral line is situated more lateral for the "wave” plate (d=5 & d=10) than for the conventional plate (d=0) in other words Yn increases. When the neutral line is available, we can compute the stresses in the bone and the plate using the following equation:


In which: y the distance to the neutral line.
I’ moment of inertia of the cross-section in relation to bending axis.

In vitro measurement of the mechanical forces acting at a fracture side in a plastic foam model


For these mechanical tests we used foam composite model in Poly-Urethane of the femur. Sawbones® (Malmo Sweden). These PU foam models have similar mechanical characteristics as real cortical bone See Table 1 and Figure 8. A conventional femur plate fixed with conventional screws was compared with a wave plate and a wave plate with a PU foam block pressed underneath the belly of the wave plate. The same was done with a femoral LCP plate. LLW (super low pressure film) Prescale Fuji Prescale film (0.5-2.5Mpa, 1Mpa= 10,2kgf/cm2), was carefully placed between the two main PU bone fragments.
The test specimens were loaded in a linear testing machine, Tinius Olsen 5K, Salfords, England Figure 9. Uniaxial non-destructive compression tests were performed at room temperature on a servo hydraulic testing machine equipped with a 5kN load cell. Unconfined compression was performed using the conventional platens test. The specimens were tested parallel to the foam rise direction. A 5-10N compressive preload was applied and the strains were set to zero. The specimens were then loaded at constant strain rate of 5mm/min. Every test specimen was tested 5 times.

Results
Intra-operative measurements with pressure sensitive film ( Fuji Prescale Film) (Table 2)
Reducing the non-union side without osteosynthesis gives a surface area of compressed prescale film (PPF) of 57.1mm2 and a pressure at rest of 1.23Mpa (174kgf), no relaxation neuromuscular blocking agents were used. After plating the femur with conventional screws the surface area of the (PPF) decreased to 57.1mm2 pressure inside the non-union was 1.19MPa (167kgf) With a bending load of 100 N the surface area of the (PPF) increased to 102.4mm2 and the pressure in the nonunion side raised to 1.21MPa (179kgf) At 300N the pressure in the non-union side fixed with a lateral plate increased to 179kgf.
When a wave plate was put on held with conventional screws the compressed area increased to 87.7mm2 the pressure recorded on the PPF was the same as the one recorded after plate osteosynthesis 1.17MPa (164kgf). With an axial load of 100N and 300N the surface area increased to 109.2mm2 and the recorded pressure was 175kgf and 179kgf respectively.

Adding a bone block underneath the wave increased the pressure contact area to 104mm2 increasing the pressure on the PPF to 1.22MPa (172kgf). The same construction loaded with a bending force of 100N decreased the recorded pressure to 167kgf and with a bending moment of 300N the recorded pressure decreased further to 157kgf.
Theoretical pressure distribution analysis of conventional and wave plate fracture fixation
The results of the calculations are shown in Table 3. These results can also be shown in an illustration depicting the relationship between the type of plate and the stresses generated in the bone and plate. (Figure 10)


In vitro measurements of the pressure distribution in site the non-union side using poly-urethane composite femur models
Under 250N uniaxial compressions in the linear testing machine of Tinius Olsen 5K we found a contact area of 33% with a conventional plate, 90% contact area with wave plate fixation and 50%. Mean pressure was 6MPa for the DCP plate, 3,5MPa for the Wave plate and 2.8MPa for the wave plate with strut graft underneath its belly. For a LCP plate under the same conditions we measured a contact area 57% with a pressure of 6.4MPa and for a wave plate locked with locked screws the contact area was 46, 3% with a pressure of 7,4MPa. Looking at the stiffness of the different constructs we calculated the secant modulus of elasticity. Ratio of stress to strain at any point on curve in a stress- strain diagram. Secant measures the total stress/strain relation Table 1. We didn't found a significant difference between a wave plate from a conventional plate and a wave plate made out of a LCP plate. Adding a bone block beneath the belly of the wave plate made the construction less stiff both with the conventional and LCP plate.
Discussion
Posttraumatic non-union of the femur varies between 0, 5% and 2, 9% for reamed and unreamed nailing [1-3]. With conventional plate osteosynthesis a non-union rate of 7, 5% to 21, 9% was reported [5,6]. These conventional plates were not intended as biological nor as an elastic osteosynthesis. With the introduction of "elastic" osteosynthesis less non-unions of the femur were seen [7,8]. The treatment of these nonunions is difficult, especially when multiple previous surgical interventions compromised the vascularisation of the fracture site. The protracted non-weight bearing of the limb will make the bone osteoporotic, which hinders a stable fixation of the femur with conventional screws.
Reamed secondary femoral exchange nailing is regarded as the procedure of choice in treating femoral diaphyseal nonunions; historically, success rates in the region of 96-100% for aseptic diaphyseal non-unions have been reported [9,10,14,15].
Reports from other authors suggested a higher than expected failure rate of exchange reamed nailing for femoral non-union [16,17]. However the use of conventional nailing systems can be challenging in other parts of the world, because of anatomical discrepancies with patients from Caucasian origin; shorter stature, narrowing IM canal. Also cost plays an increasing role. Intramedullary nails costing five times more than a conventional femur plate [18].
In the original publication of Weber [12] and Brunner [13] the "wave" plate, with its contour in the middle segment, was regarded as a bridging plate minimizing stress shielding and perfusion problems which was often seen in femur plate fixation. The bend was filled with autologous chips of cancellous bone or left open. Besides its biological advantage of less interference with blood supply in the fracture or non-union zone, required for "biological osteosynthesis" the "wave" plate also results in an improved load distribution. The usefulness of this fixation technique was shown by others such as Ring [19] and Wenzl [20]. Only Karzenis [21], in a biomechanical study comparing the rigidity characteristics of the short DCP, bridging and "wave" plates, failed to show any significant mechanical advantages of the "wave” plate technique over the "bridging” plating method.
These authors stressed the importance of lateral bone contact, only in this situation the "wave" plate was slightly stronger in mediolateral bending test (5%-10%) than that of the bridging plate. In their experiments, however, they did not include the compression mode of the tricortical strut graft beneath the contoured portion of the plate.
In our series of eight cases with a longstanding non-union of the femur, we were able to achieve bone healing in all except one case. Because of the disuse osteoporosis, cables above and below the fracture site are necessary. This technique is somewhat demanding because one needs to adjust the "wave" on the correct spot, lateral to the non-union. The "wave" must be tailored around the strut graft. One needs to get the bend right from the first time. Rebending the plate several times will weakening the plate considerably. To increase the stability of the bone-plate construct, valgus bending of the whole wave plate is essential. By bringing the plate towards the bone, considerable pressure is exerted on the iliac strut graft and non-union site.
From our theoretical analysis of the "wave" plate it becomes clear that the bend in the plate shifts the neutral axis of the bone- plate complex towards the plate. This shift results in a better loading of the cross-section of the fracture under compression. In the "normal" situation after conventional plating, the neutral axis runs more medial in the bone subjecting the lateral third of the fracture zone to tension. Cyclic tension forces inhibit, to a certain extent, the healing capacity of a fracture [22]. If there is good lateral bone contact, the "wave” plate acts as a very efficient tension band.
When the full circumferential area of the fracture can bear the load (the ideal situation) the neutral axis will be situated on 13.1mm from the centre of the femur with conventional plating. The outermost 7mm will be subjected to tension forces. In the same situation (no defect area in the fracture zone) after "wave" plating with d=10 (the distance between the contoured portion of the plate and the lateral cortex) the neutral axis will be situated on 19.1mm from the centre of the bone, where only one mm will be subjected on tension forces. Thus the "wave" plate creates a favorable mechanical situation for bone healing.
In this fracture model an assumption was made about the perfect fit of both fracture cross-sections abutting on each other, in reality this rarely happens. There will often be a gap which makes bone contact possible only after bending the plate. Even for this situation the "wave" plate exhibits a favorable mechanical behavior in comparison with the normal femur plate because there is less bending for a same amount of "fracture gap" closing, hence the "wave" plate will be subjected to less strain than the conventional femur plate.
With the ideal situation of full bone contact, situation 1, it makes not a big difference which plate you use. In this ideal situation, the normal plate takes 30.1MPa and the wave construction 22.5MPa. In the situation of nearly complete bone loss a normal plate takes 189.1MPa of load for 72.5MPa for a wave plate. From these theoretical calculations we conclude that the wave plate constructions bring more weight on the non-site and less on the plate.
Unfortunately in this theoretical analysis we are not able to substantiate the use of a strut graft to enhance the mechanical stability of the bone-”wave” plate construct. The intraoperative measurement of the pressure distribution with the pressure sensitive Fuji prescale film in one patient showed that both methods (wave and conventional plate) have a stress-shielding effect on the fracture site (-6.3% for the conventional plate & -8.4% for the "wave” plate). In mediolateral bending the pressure inside the non-union increased 4.2% for the normal plate and 12.2% for the "wave” plate.
In rest, adding a DCP plate took pressure from the nonunion side. The wave plate in rest took more pressure off the non-union side. Probably because of the elastic spring effect of the wave plate. This effect is completely abolished by adding of a bone block snuggly fitted underneath the belly of the wave plate in other words adding a bone block increased the pressure inside the non-union site.
Adding a bending moment on the non-union protected with a plate gave a slightly rise in intrafocal pressure. In other words the plate seems to take the most of the bending force. Adding a same moment force on a wave plate, redistribute considerably the pressure between the non-union side and the plate. This means an increase of pressure inside the non-union side. A bending moment at a wave plate -strut graft complex was more taken by the plate and less by the bone. This means that in these situations the adding of a bone block is less favorable for the wave plate which comes under higher tensile forces.
In our mechanical analysis on a poly-urethane femur model under uniaxial compression of 250N in a Tinius Olsen 5K linear testing machine, we found a contact area of 33% after normal plating with a pressure of 2.8MPa in the fracture side. With the wave plate nearly 90% of the PPF came under compression with a pressure of 6MPa. Wave plate with plastic block underneath the belly of the plate gave a compression area of 50% and a pressure of 3.5MPa. When we did the same set-up with a Wave plate fixed with locking screws, the results was 57% contact area and a pressure of 2.6MPa. Adding a bone block didn't change the load distribution in the fracture side less, with a contact area of 46.3% and a pressure inside the fracture of 2MPa.
The data from the three different testing’s are in concordance with each other namely the Wave plate is a more elastically constructing, loading the fracture side more. Adding a bone block underneath the belly of the plate makes the construction more stiffer taking more load than the normal wave without a strut graft. Our conclusion from these experimental observations is that the wave plate distributes more loads onto the bone and less to the implant. In a normal situation with good apposition of the bone fragments no big advance of the wave is seen. In the situation with a bone defect zone it seems a sound idea to protect the plate by creating a wave at the level of the fracture or non-union side [23-25].
In this study we could not find a definitive biomechanical advantage of adding a bone block underneath the wave of the plate. To increase the biology of these non-union autologous bone chips seems to be a better choice than a solid bone block. The in vivo measurements reported here are unique and therefore cannot be compared directly with other literature data.
References
- Eingartner C, Pütz M, Volkmann R (1997) Sekundareingriffe nach femurmarknagelung. Aktuelle Traumatol 27: 49-56.
- Strecker W, Suger G, Kinzl L (1996) Lokale Komplikationen der Marknagelung. Orthopäde, 25: 274-291.
- Hernandez-Vaquero D, Suarez-Vazquez A, Iglesias-Fernandez S, Garcia- Garcia J, Cervero-Suarez J (2012) Dynamisation and early weightbearing in tibial reamed intramedullary nailing: its safety and effect on fracture union. Injury 43(Suppl 2): S63-S67.
- Olson S, Hahn D (2006) Surgical treatment of non-unions: A case for internal fixation Injury 37(8): 681-690.
- Lies A, Scheuer J (1981) Die mediale Abstutzung-Bedeutung und Moglichkeiten der Wiederherstellung bei Osteosynthesen. Hefte Unfallheilkd 153: 243-248.
- Wagner R, Weckbach A (1994) Komplikationen nach plattenosteosynthese am femurschaft. Unfallchirurg 97(1): 139-143.
- Stuürmer KM (1996) Die elastische plattenosteosynthese, ihre biomechanik, indikation und technik im vergleich zur rigiden osteosynthese. Unfallchirurg 99(11): 816-829.
- Schmidtmann U, Knopp W, Wolff C, Sturmer KM (1997) Ergebnisse der elastischen Plattenosteosynthese einfacher Femurfrakturen beim Polytrauma. Unfallchirurg 100: 949-956.
- Court-Brown CM, Keating JF, Christie J, McQueen MM (1995) Exchange intramedullary nailing. Its use in aseptic tibial non-union. J Bone Joint Surg Br 77(3): 407-411.
- Okhotsky VP, Souvalyan AG (1978) The treatment of non-union and pseudarthrosis of the long bones with hick nails. Injury 10(2): 92-98.
- Reynders P (2000) Pressure plate fixation according to Brunner & Weber for recalcitrant pseudarthrosis of the femur. Folia Traumatologica Lovaniensia, Leuven, Belgium, pp. 148-156.
- Weber BG, Cech O (1976) Pseudarthrosis, pathophysiology, biomechanics, therapy and results.
- Brunner CH, Weber BG (1981) Besondere Osteosynthese-techniken. Springer-Verlag. Berlin- Heidelberg-New-York, USA, p. 46-62.
- Oh I, Nahigian SH, Rascher JJ, Farrall JP (1975) Closed intramedullarynailing for united femoral shaft fractures. Clin Orthop 106: 206-215.
- Webb LX, Winquist RA, Hansen ST (1986) Intramedullary nailing and reaming for delayed union or nonunion of the femoral shaft. A report of 105 consecutive cases. Clin Orthop 212: 133-141.
- Weresh JM, Hakanson R, Stover MD, Sims SH, Kellam JF, et al. (1999) Failure of exchange reamed intramedullary nails for ununited femoral shaft fractures. J OrthopTrauma 4(5): 335-338.?
- Banaszkiewicz PA, Sabboubeh A, McLeod I, Maffulli N (2003) Femoral exchange nailing for aseptic non-union: not the end to all problems. Injury 34(5): 349-356.
- Angelini AJ, Livani B, Flierl MA, Morgan SJ (2010) less invasive percutaneous wave plating of simple femur shaft fractures: A prospective series. Injury 41(6): 624-628.
- Ring D, Jupiter JB, Sanders RA, Quintero J, Santoro VM, et al. (1997) Complex nonunion of fractures of the femoral shaft treated by "wave"- plate osteosynthesis. J Bone Joint Surg 79B: 289-294.
- Wenzl ME, Wolter D, Fuchs S, Kortmann HR, Jurgens C (1999) Druckplattenfixateur interne fur das Femur, ein winkelstabiles Implantat. Klinische Ergebnisse der Behandlung von Pseudarthrosen, Refrakturen, posttraumatischen Fehlstellungen und Frakturen. Trauma Berufskrankh 1(4): 344-350.
- Karnezis IA (2000) Biomechanical considerations in "biological" femoral osteosynthesis: an experimental study of the "bridging" and "wave” plating techniques. Arch Orthop Trauma Surg 120(5-6): 272275.
- Augat P, Merk J, Wolf S, Claes L (2001) Mechanical stimulation by external application of cyclic tensile strains does not effectively enhance bone healing. J Orthop Trauma 15(1): 54-60.
- Weber BG, Cech O (1976) Pseudoarthrosis. Bern: Hans Huber, Switzerland, pp. 181-184.
- Li B, Aspden RM (1997) Composition and mechanical properties of cancellous bone from the femoral head of patients with osteoporosis or osteoarthritis. J Bone Miner Res 12(4): 641-651.
- Kelly N, McGarry JP (2011) Experimental and Computational Characterization of the Elasto-Plastic Properties of a Polyurethane Trabecular Bone Analogue. National University of Ireland, Galway, Ireland.















