




Knowledge on Sexual and Reproductive Health among Young People in a Selected Community
SM Monwar Hossain1*, Yeasmin Ara2, Md Ashrafuzzaman1, Md Rashed Miah1, Md Ruhul Amin1 and Satya Prio Dhar3
1Master of Public Health, ASA University Bangladesh, Bangladesh
2Master of Social Science in Health Economics, University of Dhaka, Bangladesh
3Master of Public Health, Northern University Bangladesh, Bangladesh
Submission: September 21, 2016; Published: September 30, 2016
*Corresponding author: S.M. Monwar Hossain, Master of Public Health, ASA University Bangladesh, Bangladesh.
How to cite this article: SM Monwar H, Yeasmin A, Md Ashrafuzzaman, Md Rashed M, Md Ruhul A, et al. Knowledge on Sexual and Reproductive Health among Young People in a Selected Community. J Gynecol Women’s Health. 2016; 1(3): 555565. DOI: 10.19080/JGWH.2016.01.555565
Abstract
A cross sectional descriptive study was conducted among 215 young people from January to May 2016. Respondent were selected form Bogra district mostly who were studying in Bogra Azizul Hoque College and age group 18-24 years and who were living that area. Semi structured questionnaire was employed as instrument for data collection. I used liker scale i.e. Poor Knowledgeable, Moderate knowledgeable, fully knowledgeable. Total mark was 5 and I took 5 was fully knowledgeable, 3-4 was moderate knowledgeable and below 3 was poor knowledgeable. Mean age of the participants was 20 years. Among 215 participants the educational background 133 (61.9%) hold HSC and above, 47 (21.9%) hold SSC, 25 (11.6%) were up to SSC. Among the total participants 215 (N=215) the higher number of participants 56.3% (n=121) were moderate knowledgeable. On the other hand, 41.4% (n=89) were poor knowledgeable and 2.3% (n=5) were fully knowledgeable. There was significance (p= 0.000) association between sex and knowledge level of the participants.
Keywords: Knowledge; Sexual health; Reproductive health; Young people
Introduction
Adolescence is a profound and complex stage of life that influences future health outcomes, attitudes, and behaviors [1]. The environmental impact on adolescent health and development is clearly seen in the slums [2]. Of the one billion young people worldwide, most still lack adequate reproductive health care. Programs to give youth the information and means to protect themselves against unwanted pregnancy and sexually transmitted infections often face resistance because they challenge deeply held cultural beliefs about sex, parenting, and the roles that men and women play [3]. Knowledge on sexual and reproductive health is very much necessary to tolerable MMR and IMR in any country. Since Bangladesh is developing country. Premarital sex and extra marital sex is prohibited and people don’t take easily the term sex being social taboo. The study helps to depict the actual scenario regarding the knowledge level SRH issue among the young group. So that the respective authority can take intervention to reduce the consequence according to the lack of SRH knowledge.
Methodology
Study design: Cross sectional descriptive study
Study area: The study was carried out in the Bogra district. The study was conducted among those who are belonging the age of 18-24 Years old mostly student in Bogra district. A total of 215 participants were purposively selected for the interview.
Study period: The study was carried out within the time period of January to May 2016.
Study population: People who were belonging the age 18-24 are included in the study, mostly college going student.
Inclusion criteria
- Respondents whose age ranges were 18-24
- Respondents who were willing to participate
Sample size: However, due to time and resource limitation I had taken 215 samples in my study
Sampling technique: None probability purposive sampling technique was used to carry out the data collection.
Data collection technique: A structured question was used to collect the data. Question was divided into two sections. First section included the socio demographic data included class, age, sex, religion, family size, education of responded as well as guardian of the family who was main earning person included their occupation. The second section included 32 questions regarding the knowledge level on the SRH. A total of 43 question set up for this study. Individual interview was utilized which was directed by researcher and two assistants after explaining the study of this study and obtaining written informed consent. The questionnaire was developed both in Bangla and English. A pilot test was performed within a small group of the probable responded.
Data analysis: All statistical analysis was performed using SPSS 16.0 for Windows (SPSS, Inc, Chicago, II,). Frequency distraction was computed for demographic variables.
Ethical consideration:
- Inform decision making consent was taken before the interview
- The interview was carried out separately to each respondent to ensure proper concentration
- Commitment had been given to maintain confidentiality
- Time was taken from the respondent before conducting the interview
- Not any force applied to respondents to participate in this study
- Data were collected using appropriate method
- All interviews were conducted in the local language to ensure accuracy and consistency
- Questionnaires were frequently checked after completing the interview
- The data was noted very carefully and systemically
- The privacy of the respondent was strictly maintained
Scoring knowledge: I had taken a total 5 questions to assess the knowledge level of the participants to SRH. I used liker scale i.e. Poor Knowledgeable, Moderate knowledgeable, fully knowledgeable. Total mark was 5 and I took 5 was fully knowledgeable, 3-4 was moderate knowledgeable and below 3 was poor knowledgeable.
The question was mentioned below
- Who is the decision maker for having child?
- Do you know the legal age of marriage for male and female?
- Do you know about the consequence of early pregnancy?
- What do you mean about the recognition of the choice to marry?
- What is the reproductive age of woman?
Results
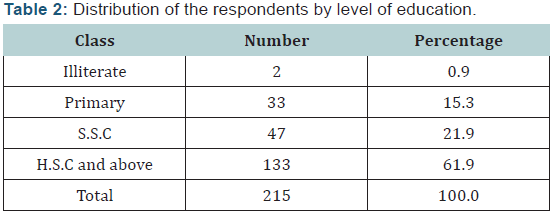
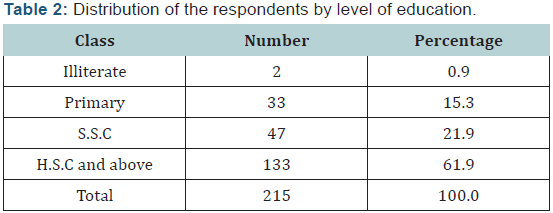
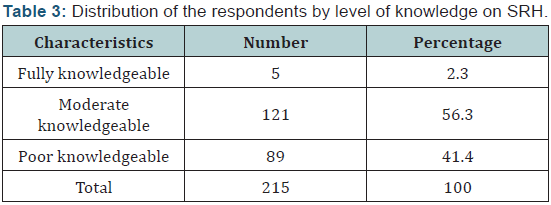

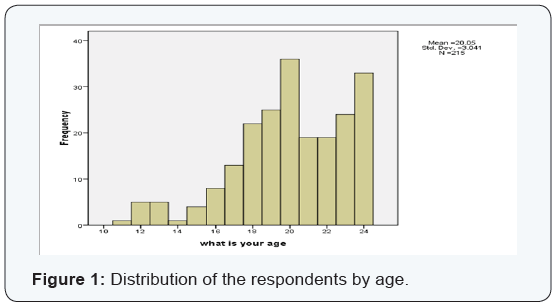
Among 215 participants, 68.8% (n=148) were found male in contrast to other responded of Female and other (hijra) were 29.8% (n=64) and 1.4% (n=3) respectively (Table 1). Among the total number of participants (n=215) maximum age group was 20 (n=36) where the mean, Std. Dev was 20.05 and 3.041 respectively (Figure 1). Among 215 participants, 61.9% (n=133) were in HSC and above, in contrast to other respondent’s level of S.S.C were 21.9% (n=47), primary level was 15.3% (n=33) and 0.9% were illiterate (n=2) (Table 2). Among the total participants 215 (N=215) the higher number of participants 56.3% (n=121) were moderate knowledgeable. On the other hand, 41.4% (n=89) were poor knowledgeable and 2.3% (n=5) were fully knowledgeable (Table 3). Among the all respondents highest number of them was male 68.83% (n=148) among them 2.70% (n=4) were fully knowledgeable and 61% (n=91 were moderate knowledgeable to SRH. Female respondents were 29.76% (n=64) among them 46.87% were moderate knowledgeable to SRH. There was a positive and significance (p<0.05) association age and knowledge (Table 4).
Discussion
Majority of the participants 61.9% (n=133) education level were HSC and above. Among the all participants 38.8% had good knowledge on SRH. On the other hand, majority number of participants 54.9% (n=118) didn’t have the SRH knowledge. It is not only that youth lack adequate information and suffer from the taboo surrounding SRH issues, but the low social status and the lack of rights of women also seriously hamper them in making decisions to protect themselves from sexual and reproductive health problems and unwanted pregnancies. Violence against women is accepted in all layers of society and rape, acid throwing, harassment, forced prostitution and trafficking are on the rise. Domestic violence remains the biggest threat facing adolescent girls. Reproductive health rights ensure that people are able to have satisfying and safe sex life and that they have the capacity to reproduce with freedom to decide, when and how often to do so. Reproductive health rights also include the access of women to high quality health care services that help in protecting women during pregnancy and childbearing and providing the couples with the best chances of having healthy. In addition, reproductive health rights might be an important indicator for women’s health. A study was done to assess knowledge, perception, attitude, and practices of reproductive health rights among the Palestinian women of reproductive age (15-49) and the results of the study revealed that women had positive understanding of their reproductive health rights. Women mentioned the right to have good access to health care during and after the course of pregnancy as their first important right. The majority of women were able to identify the modern contraceptives and most women mentioned that they made the fertility decision together with their husbands which was similar to my study. Women started antenatal care at a relatively early stage of their pregnancy (before 4-month pregnancy), and 78.2 percent of women made six or more antenatal care visits during their entire pregnancy but present study found that most of the respondents made three or four antenatal care visits during their entire pregnancy which was dissimilar to Palestine study. Based on the results of that study, it was recommended to consider these results when planning for any women’s health programs and projects. In order to improve health care services based on women’s needs and priorities, they also recommended setting new policies and regulations that protect women against violence and organizing public education programs to change women’s perception towards intimate partner violence. Empowering women through education and open employment opportunity might help women in making decisions regarding their fertility and taking an active role when they experience any reproductive health rights violation [4]. A study was done to understand the family planning (FP) knowledge and current use of contraception and its predictors among women of the Mru people – the most underprivileged indigenous community in Bangladesh. Only about 40% of respondents had ever heard FP messages or about FP methods – two-fifths of the national figure (99.9%). The current use of contraception was much lower (25.1%) among the Mru people than at the national level (55.8%). Among both modern and traditional methods, the contraceptive pill ranked first. About two-thirds (66.0%) of married women used this method – more than two times than the national figure (28.5%). On the other hand, the prevalence of male methods was comparatively lower than at the national level. Logistic regression models revealed that place of residence, religion, age, school attendance, husband’s school attendance, service provided in the community, distance to the service center, and exposure to mass media had significant effects on knowledge of FP and on use of contraception. Education for mothers and vernacular language-based doorstep FP programs with special emphasis on awareness were suggested for the community [5]. A comparative case study was done in Nepal on safe motherhood practice and they showed that more than a half have knowledge about safe motherhood but practice is found lower as compared to the magnitude of known. Antenatal care is found better in comparison about safe motherhood is found some increased now than before. Family planning knowledge is found better as compared to antenatal, safe delivery and postnatal cares among this caste [6]. Sexual and Reproductive rights and health for the women of Asia sometimes appears to be a distant vision. The ICPD, the Millennium Development Goals and the Beijing Declaration notwithstanding, maternal mortality continues to be high in many parts of Asia and patriarchal society structures reinforce women’s lack of autonomy and decision making capacities thus putting their lives at risk on a daily basis through deprivation, physical and sexual violence, rape, unsafe abortions, and others. Unsafe abortions still contribute to 13-50 % of the maternal mortality in some of these countries. Only three respondents have actually dealt with abortion related cases. A few respondents said that they have dealt with issues like adultery, extra marital relations etc. but not with abortions. The source of their information on abortion was therefore media or other reports and TV as like my study subjects. However, seventeen of them were interested in knowing more about abortion and abortion laws [7]. A study was done aims at identifying the effect of birth spacing on maternal health among 324 married women at the fertile age period and revealed that women practicing birth spacing were 33.3% of the studied sample. Good knowledge and favorable attitude were 88% and 100% of properly birth spaced women. Rural origin women were less practicing birth spacing [8].
Conclusion
In summery the level of knowledge seems to have a significant relation with sex. More than half of the respondents had moderate knowledge on SRH and rest of the participants had poor knowledge.
References
- Sawyer SM, Afifi R, Bearinger L, Blakemore SJ, Dick B, et al. (2012) Adolescence: A Foundation for Future Health. Lancet 379(9826): 1630-1640.
- Cortez R, Hinson L, Petroni S (2014) Adolescent Sexual and Reproductive Health in Dhaka’s Slums, Bangladesh. HNP Discussion Paper. The World Bank, Washington, DC, USA 1: 1-4.
- Yotchou APT, Gersainde NEM, Njouomegne S (2013) Adolescent Sexual Reproductive Health Care. Abstracts of Poster Presentations, The European Journal of Contraception & Reproductive Health Care 18(Supply 1): S90-S264.
- Dhaher E (2008) Bielefeld (Germany): Bielefeld University. Reproductive health human rights: women‘s knowledge, attitude, and practices toward their reproductive health rights in Palestine.
- Islam MR, Thorvaldsen G (2012) Family planning knowledge and current use of contraception among the Mru indigenous women in Bangladesh: a multivariate analysis. Open Access Journal of Contraception 3: 9-16.
- Khima Oli (2007) Safe motherhood prctices in Rukum. Tribhuvan University, Kirtipur, Nepal.
- Anika R, Laura K, Stanley KH (1998) A Global Review of Laws on Induced Abortion, 1985-1997. Int Fam Plann Persp 24(2): 56-64.
- el- Maaddawi Y, Aboul-Ella MN, Abdel-Moneim MN, Tantawy AB (1992) Study of the effect of birth spacing on maternal health. J Egypt Public Health Assoc 67(5-6): 725-729.
