




Value of Urocortin as a Marker for Preterm Labor
Mourad MohiELdinELsaeid1, Haitham Abdel Mohsen Sabaa* and Hani MohamudMehanna
Department of Obstetrics and Gynecology, Ain Shams University, Egypt
Submission: May 10, 2016; Published: May 25, 2016
*Corresponding author: Haitham Abdel Mohsen Sabaa, Lecturer of Obstetrics and Gynecology, Faculty of Medicine, Ain Shams University, El-Abaseya, Naser City, Cairo, Egypt, Tel: 0201227333924; Email: profhaithamsabaa@gmail.com
How to cite this article: Mourad M E E, Haitham A M S, Hani MM. Value of Urocortin as a Marker for Preterm Labor. J Gynecol Women’s Health. 2016; 1(2): 555559. DOI: 10.19080/JGWH.2016.01.555559
Abstract
Introduction: Preterm delivery is responsible for considerable neonatal morbidity and mortality, accurate predication could decrease such complications different biological markers have been suggested to predict preterm labor, maternal plasma urocortin level was suggested as a marker.
Methods: 100 women diagnosed with threatened preterm labor were included in the study and their blood level of urocortin was measured at admission time and its level was correlated with the occurrence of established preterm labor.
Results: The best cutoff criterion of plasma urocortin level was more than 365.2 pg/ml with sensitivity at 87% (CI: 73.7 – 95.1) and specificity of 100% (CI: 93.4 – 100). Followingly the positive predictive value for this cutoff point (>365.2 pg/ml) was 100% (CI: 91.2 – 100) & the negative predictive value was 90% (CI: 79.5 – 96.2).
Conclusion: Our study showed that maternal plasma urocortin can be used for prediction of preterm delivery as an independent factor.
Keywords: Urocortin; Prediction; Preterm; Labor
Introduction
Preterm labor is the single most important complication of pregnancy in the absence of congenital abnormality, as it is recognized as a worldwide problem responsible for more than 80% of neonatal deaths and more than 50% of long term morbidity in the surviving infants [1]. Recent screening strategies for preterm delivery have focused on early identification of patients at risk, enable an earlier intervention for preterm labor. That is why it was extremely important to establish a reliable predictor for preterm birth to plan the management strategy.
The use of biologic markers to enhance clinical accuracy in predicting preterm birth and to identify those women at risk has been proposed In this context, placenta and fetal membranes are key tissues in the response to infection and in activating the inflammatory pathways leading to PTD through the up-regulation of chemokines, cytokines, and corticotropin releasing hormone (CRH), which involves urocortins as well [2]. Urocortin – a novel peptide of the corticotrophin releasing factor family is expressed by gestational tissues such as amnion, chorion, decidua, trophoblast, and myometrium and is measurable in maternal and fetal circulation showing stable concentrations in maternal plasma from the first to third trimesters of pregnancy [3]. The aim of this study is to evaluate maternal urocortin level as a predictive value in pregnant women with threatened preterm labor.
Patients and Methods
This prospective study was conducted partially at Ain Shams University Maternity Hospital and El-Galaa Maternity Teaching Hospital after approval of the research and ethics committee during the period from December 2013 until January 2015. This study included 100 pregnant women with singleton pregnancies between 28 and 34 completed weeks of gestation that have been diagnosed with threatened preterm labor and who had consented to participate in this study.
All patients were subjected to: A detailed history abdominal examination to assess uterine contractions and their regularity if present as well as to assess the fundal level. P/V examination was done to assess the cervix regarding dilatation or effacement levels as well as to check for intactness of membranes. Ultrasound upon admission to confirm: Gestational age, Amount of liquor, Singleton pregnancy, Presence of any fetal anomalies. All Patients involved in this study fulfilled the following criteria: age between 18-35 years, gestational age from 28 weeks to 34 weeks confirmed by sure history of last menstrual period and first trimestric ultrasound, singleton pregnancy. Criteria for threatened preterm labor in according to Creasy and Herron criteria of preterm labor: The diagnosis of preterm labor should be made if uterine contractions occur at a frequency of four per 20 minutes or eight per 60 minutes and are accompanied by one of the following: PROM, cervical dilatation greater than 2cm, effacement exceeding 50 percent or a change in cervical dilatation or effacement detected by serial examinations [4]. Excluded from the study: Pregnant women with history of any medical or systemic diseases, patient with risk factors as polyhydramnios, past history of preterm labor, multiple pregnancy.
All patients were notified by the nature of this study and verbal consents were obtained from the patients prior to involvement upon admission into the Maternity Hospital. All women who are diagnosed with threatened preterm labor (28 - 34 weeks) were enrolled in this study. Serum samples were collected from all women before any intervention such as tocolysis or administration of steroids. All women were sampled once at the time of admission. Routine laboratory investigations included complete blood count using Sysmex21 k, C reactive protein using latex agglutination test and complete urine analysis. Samples of 10 ml blood will be collected from each subject: 2 ml of which will be put on EDTA to perform CBC and 3 ml will be left to clot, serum obtained will be collected and the remaining laboratory test will be performed.
Blood samples were collected in a chilled 4 ml heparinized monovette and gently mixed several times. The samples were then transferred to a centrifuge tube and were centrifuged at 1600 rpm for 15 min at 4 °C. The supernatant was then removed and if precipitation appeared, a second round of centrifugation occurred. Plasma samples were stored at −70°C until assay. Urocortin concentrations were then measured using ELISA. The range of the urocortin assay kit is 1nmol/L - 50nmol/L. This took place in the biochemistry department in Ain Shams University.
Urocortin measurement: plasma urocortin level will be assayed using EIA kit (phoenix pharmaceutical) according to the manufacturer instructions. We will add calibrators and samples (50μl) to 96 well immune plates coated with biotinylated goat anti-rabbit IgG (Capture antibodies). We then add 25 μl of rabbit polyclonal antihuman urocortin serum (detection antibody) and an equal volume of biotinylated antibody to each well will be added and incubated the plate for two hours at room temperature. The well will be washed with assay buffer, and streptavidin conjugated horseradish peroxidase will be added, and again will be incubated for 1 hour at room temperature. The well will be washed with substrate solution (3, 5, tetramethylbenzidine) and will be incubated for 1 hour at room temperature. The reaction will be stopped by adding 2mol/l HCL and the absorbance will be read at 450 nm. Quantification of the unknown samples will be achieved by comparing their absorbance with a reference curve prepared with known standard concentrations.
Statistical Methods
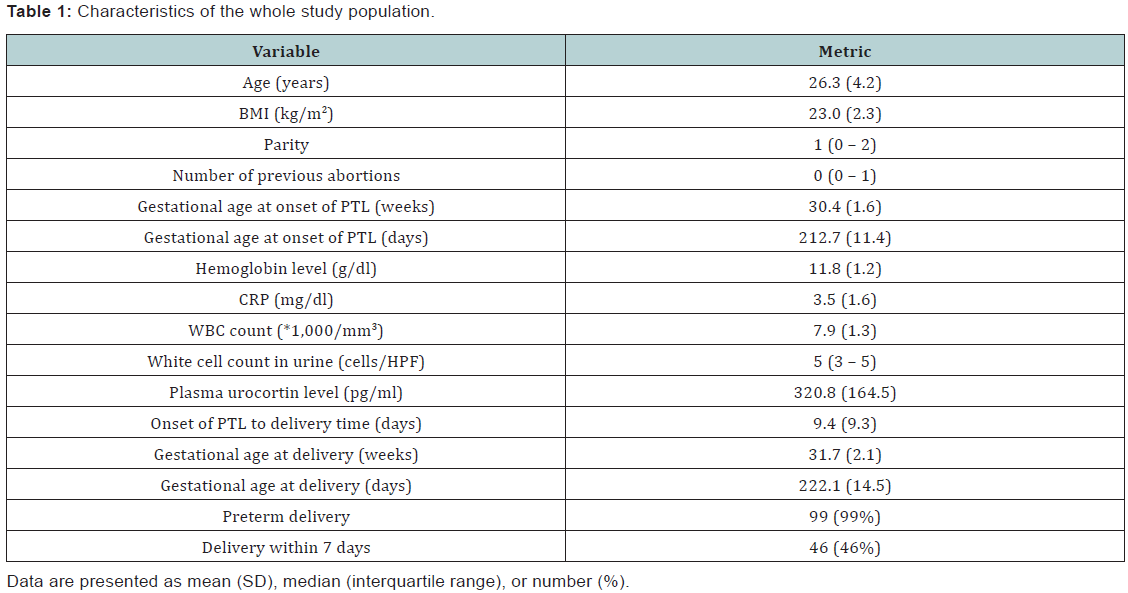
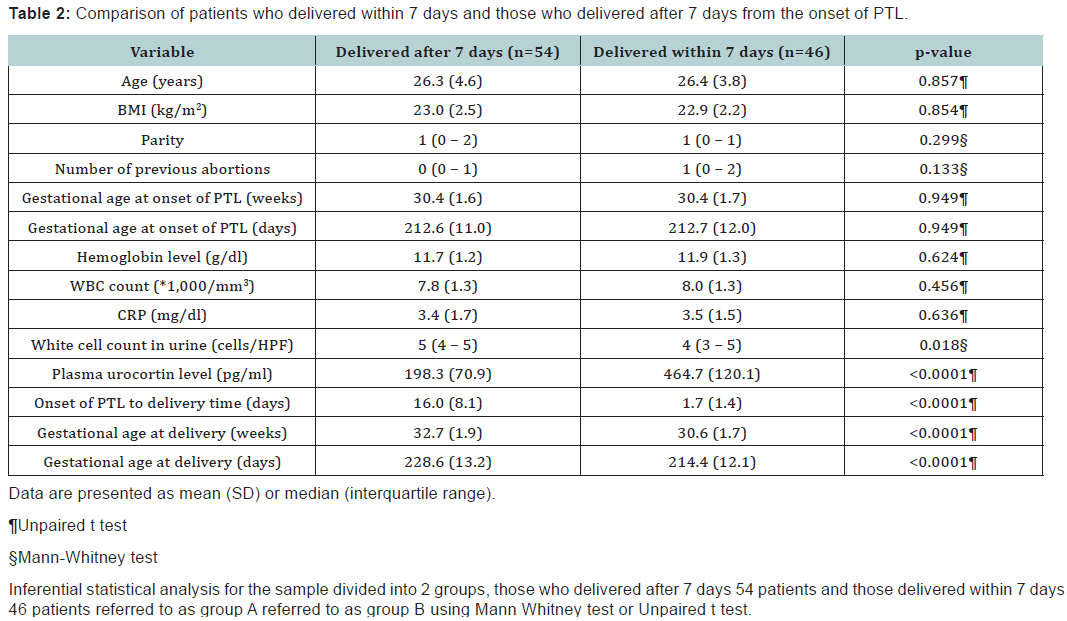
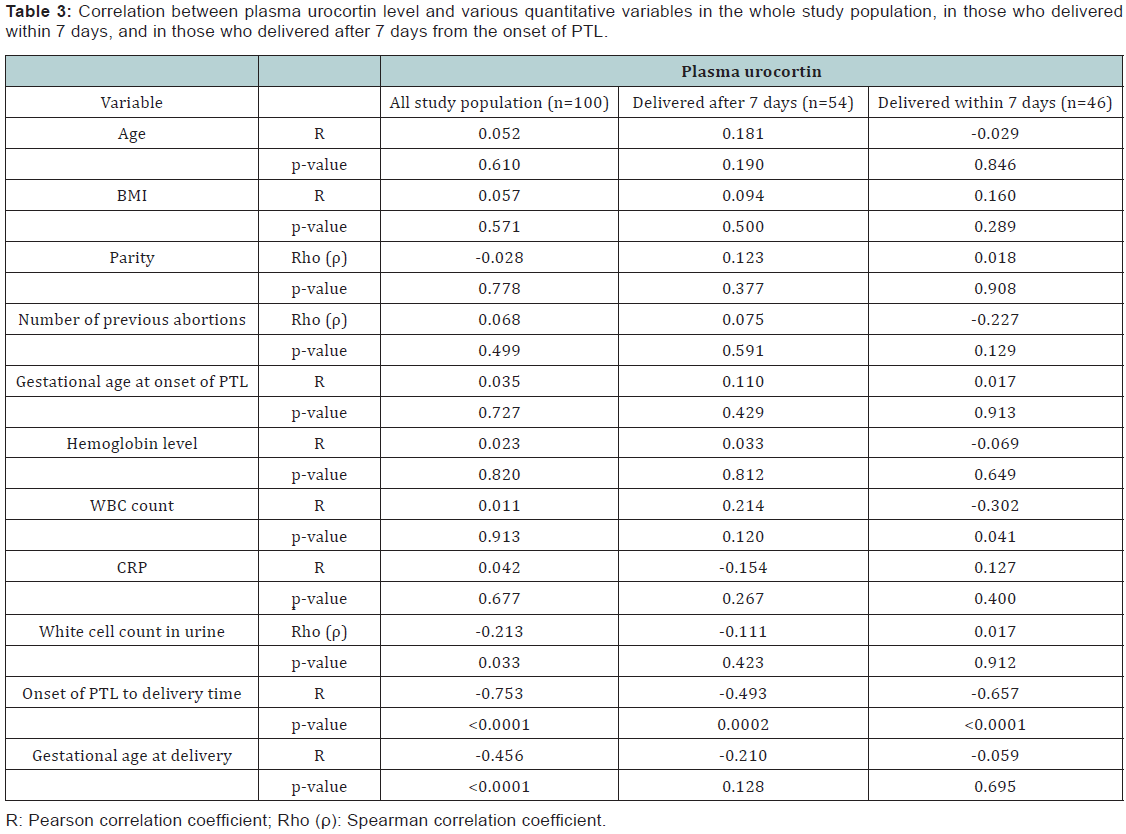
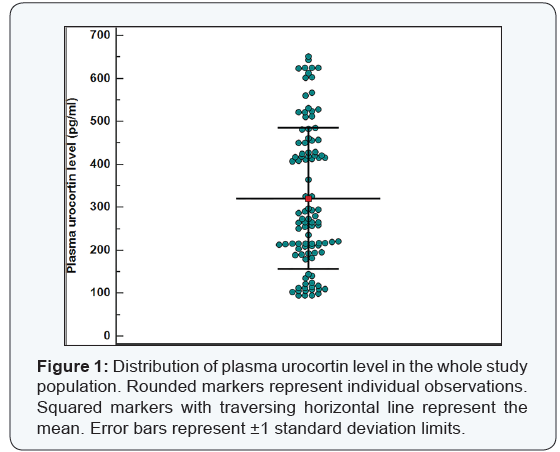
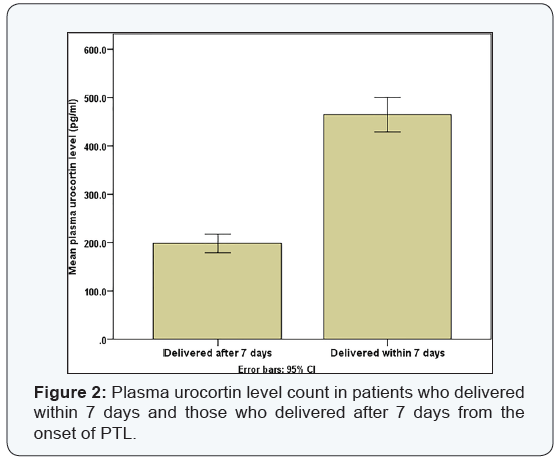
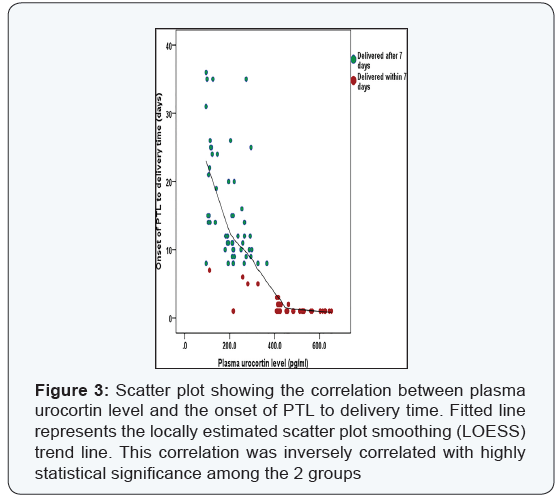
Data were analyzed using IBM© SPSS© Statistics version 22 (IBM© Corp., Armonk, NY, USA) and MedCalc© version 14 (MedCalc© Software bvba, Ostend, Belgium). Demographic criteria of the studied group are shown in Table 1, The analysis using unpaired T test revealed that there was no statistical significant difference between the 2 groups (p = 0.8) as shown in Table 2. The plasma urocortin level among the sample had a mean 320 pg/dl with standard deviation of 164.5 as shown in Figure 1. The plasma urocortin level showed highly statistical significant difference (p<0.000) group A had a mean of 198.3 ± 70.9 while group B had a significantly higher mean 464.7 ± 120 pg/ml, (Figure 2). There is an inverse correlation between plasma urocortin level and the onset of PTL to delivery time and it is highly significant (Figure 3 & Table 3). The ROC curve analysis was done using DeLong method to assess the prediction power of plasma urocortin level, CRP level & WBC for the delivery within 7 days. Only the Plasma Urocortin level showed significant ROC curve with high area under the curve (p<0.000, AUC=0.9) with confidence interval of 0.9 to 1.
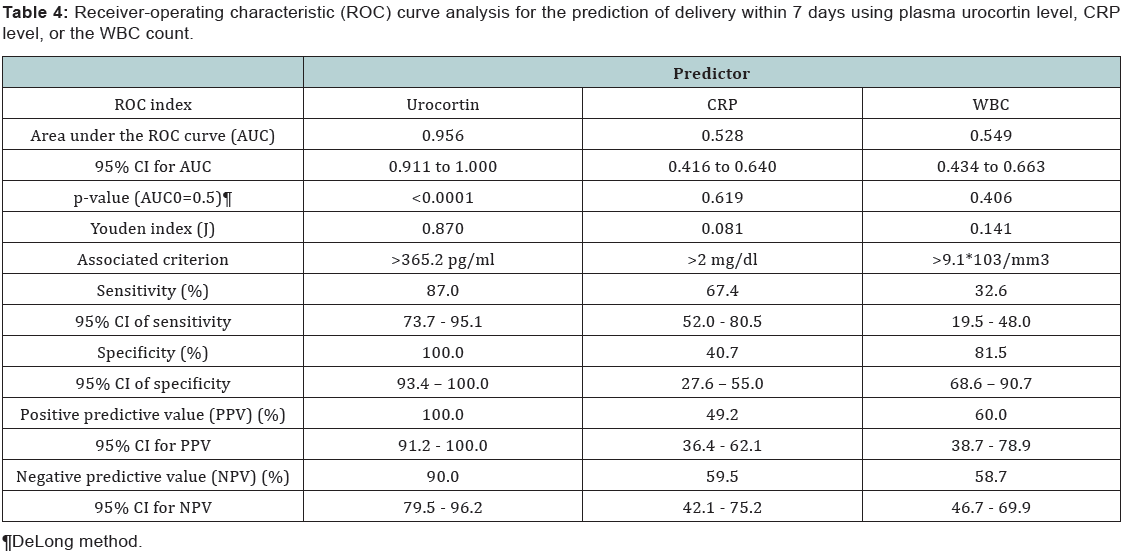
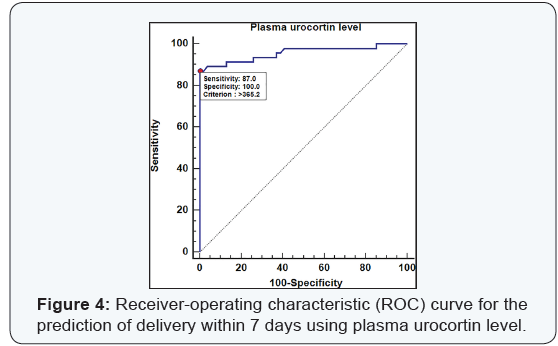
The best cutoff criterion of plasma urocortin level was more than 365.2 pg/ml with sensitivity at 87% (CI: 73.7 – 95.1) and specificity of 100% (CI: 93.4 – 100). Followingly the positive predictive value for this cutoff point (>365.2 pg/ml) was 100% (CI: 91.2 – 100) & the negative predictive value was 90% (CI: 79.5 – 96.2). The CRP level & WBC count level didn’t have any significant ROC curve (p=0.6 & p=0.4) for the prediction of the delivery within 7 days (Table 4). The cutoff point of plasma urocortin level was more than 365.2 pg/ml with sensitivity at 87% (CI: 73.7 – 95.1) and specificity of 100% (CI: 93.4 – 100). Followingly the positive predictive value for this cutoff point (>365.2 pg/ml) was 100% (CI: 91.2 – 100) & the negative predictive value was 90% (CI: 79.5 – 96.2). The ROC curve for the plasma urocortin level had an area under the curve of 0.956 with highly statistical significance p<0.000 (Figure 4).
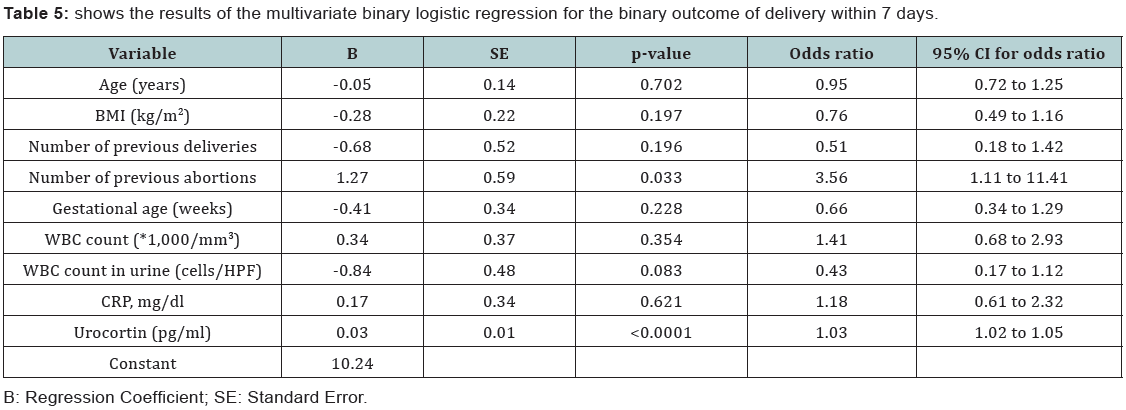
The age in years, BMI, number of previous deliveries, the gestational age in weeks, the WBC count and WBC count in urine, CRP level were all insignificant predictors for the delivery within 7 days. The number of previous delivery had a significant statistical prediction power for the delivery within 7 days (p=0.03) the Beta coefficient as 1.27. The odds ratio of number previous delivery was 3.56 (CI: 1.11 – 11.41) .The plasma urocortin level had a statistical highly significant prediction power for the delivery within 7 days (p<0.000) the Beta coefficient was 0.03. The odds ratio of the plasma urocortin level was 1.03 (CI: 1.02 to 1.05) (Table 5).
Discussion
This prospective study conducted at both Ain Shams University Hospital & El-Galaa Maternity Hospital was done to measure the maternal plasma urocortin level evaluate its accuracy in predicting preterm delivery in women with threatened preterm labor. The preterm delivery occurred in 99 patients (99%) and the delivery within 7 days occurred in 46 patients (46%). The ROC curve analysis was done using DeLong method to assess the prediction power of plasma urocortin level, CRP level & WBC for the delivery within 7 days. Only the Plasma Urocortin level showed significant ROC curve with high area under the curve (p<0.000, AUC=0.9) with confidence interval of 0.9 to 1.
The best cutoff criterion of plasma urocortin level was more than 365.2 pg/ml with sensitivity at 87% (CI: 73.7 – 95.1) and specificity of 100% (CI: 93.4 – 100). Followingly the positive predictive value for this cutoff point (>365.2 pg/ml) was 100% (CI: 91.2 – 100) & the negative predictive value was 90% (CI: 79.5 – 96.2). The CRP level & WBC count level didn’t have any significant ROC curve (p=0.6 & p=0.4) for the prediction of the delivery within 7 days.
The ROC curve using DeLong method for the CRP level didn’t show any statistical significant curve (p=0.6) and the area under curve was 0.52. The sensitivity was 67.4% (CI: 27.6 – 55) & the specificity was 40.7% (CI: 36.4 – 62.1) at more than 2 mg/ dl. Similarly the ROC curve for the WBC count didn’t show any statistical significant curve (p=0.4) and the area under the curve was 0.54. The sensitivity was 32.6% (CI: 19.5 – 48) and the specificity was 81.5% (CI: 68.6 – 90.7) at more than 9.1 *103 / mm3.
The results of the multivariate binary logistic regression for the binary outcome of delivery within 7 days showed that the age in years, BMI, number of previous deliveries, the gestational age in weeks, the WBC count and WBC count in urine, CRP level were all insignificant predictors for the delivery within 7 days. The number of previous delivery had a significant statistical prediction power for the delivery within 7 days (p=0.03) the Beta coefficient as 1.27. The odds ratio of number previous delivery was 3.56 (CI: 1.11 – 11.41). The plasma urocortin level had a statistical highly significant prediction power for the delivery within 7 days (p<0.000) the Beta coefficient was 0.03. The odds ratio of the plasma urocortin level was 1.03 (CI: 1.02 to 1.05).
To conclude, our study showed that maternal plasma urocortin can be used for prediction of preterm delivery as an independent factor. Even after adjusting the study and taking into consideration other factors that could influence the area under the curve. Our study still showed high predictive powers, and with the use of those other factors a better predictive outcome was achieved. The study of Florio et al. [5] was conducted for the prediction of preterm delivery based on maternal plasma urocortin. The study measured the plasma levels of urocortin in women with threatened preterm labor to evaluate whether the measurement may predict preterm labor. This observational study included 85 women with singleton pregnancies between 28-34 completed gestational weeks with threatened preterm labor and the pregnancy outcome and evaluation of sensitivity, specificity, and predictive values of urocortin as a diagnostic test for preterm delivery were measured. Thirty of the 85 patients (35.3%) had preterm delivery within 7 days from admission, whereas the remaining delivered later. Urocortin was found to be significantly higher in women who delivered preterm (median 131.2pg/ml, with an interquartile interval of 115.1-139.4 pg/ml) than those who progressed to term delivery (median 95.4pg/ml, with an interquartile interval of 124.8 – 141.2 pg/ml). Receiver operating characteristic curve analysis revealed that urocortin at the cut-off of 113.9 pg. /ml had sensitivity of 80% & specificity of 100%, positive predictive value of 100%, and negative predictive value of 90% as a marker for preterm delivery. The conclusion was that maternal plasma urocortin concentration is increased in patients with threatened preterm labor, who have preterm delivery, and its measurement may be a promising new biochemical marker of preterm delivery [3,5].
Abdullah et al. [6] conducted a study that focused on amniotic fluid urocortin-1 concentrations for the prediction of preterm delivery. The aim of this study was to analyze whether urocortin-1 concentrations in midtrimester amniotic fluid could serve as an indicative marker of preterm labor. This was a retrospective cohort study that measured urocortin-1 concentrations in midtrimester amniotic fluid of 22 pregnant women with preterm deliveries and 45 women who delivered at term using enzyme-linked immunosorbent assay. This is similar to our study in that the urocortin was also measured using the enzyme-linked immunosorbent assay. The median amniotic fluid urocortin-1 concentration was significantly lower in the women with preterm birth (40.06 pg/ml; range 13.77-67.58) than in the women who gave birth at term (49.56 pg/ml; range 26.25-175.9 pg/ml; P = 0.022). The study showed a sensitivity of 81.8%, specificity of 40.0%, and a positive predictive value of 40%. These results show that low urocortin-1 concentration in midtrimester amniotic fluid could be used as an indicative marker of preterm birth. This finding is coherent with our study regarding the fact that urocortin can be used as a predictive marker for preterm delivery, but differs somewhat regarding the values. These findings suggest that the lower the urocortin-1 concentrations in the amniotic fluid (<40.06 pg/ml), the higher the chance for preterm delivery to occur.
Another study was done by Iavazzo et al. [7]. This was a general study that aimed to assess the role of urocortin in gynecological and obstetrical conditions. The study objective was to assess the possible role of urocortin in different conditions, which included preterm labor. This study involved conducting a MEDLINE search that was commenced with the terms “urocortin” “preterm labor” “placenta” “plasma” “amniotic fluid”. Seventy-three articles were found to be relevant on the field and the potential role of urocortin in those conditions was presented. The amounting data derived from these articles suggested that urocortin could play a significant role in maintenance of placental function and labor. It was noted that further investigation on the field is necessary in order to confirm. For example, McLean et al. proposed the theory of the ‘CRH placental clock’ which could determine the duration of gestation and the timing of parturition & delivery [8]. Also, Torricelli et al. [9] revealed that levels of CRF & urocortins were lower when comparing post-term with term pregnancies out of labor. In conclusion, the data suggested that urocortin could play a significant role in human reproduction as well as in initiation, maintenance, and termination of pregnancy. Urocortin was found to have a major role in human placenta by stimulating ACTH, prostaglandins, and activing a secretion and by regulating placental vessel resistance to blood flow. It was evident by Glynn et al. [10], that levels of maternal plasma urocortin were higher at labor than those during pregnancy, and for that reason they suggested that urocortin is involved in the mechanisms of labor by promoting myometrial contractility. They concluded that urocortin provided a high predictor for the duration of gestation, and that further investigation on the field is necessary to clarify the physiological pathways in which this molecule participates. These findings are coherent with our study.
Our limited study showed that plasma urocortin can indeed be used as a predictive marker for preterm labor with a good predictive value as evidenced by a significant area under the ROC curves. Our study helped us conclude that urocortin can be used as an independent factor or in combination with other statistically significant factors to help in the prediction of preterm delivery. Even after adjusting the study and taking into consideration other factors that could influence the area under the curve, our study still showed high predictive powers for the urocortin as an independent factor for preterm delivery prediction. Urocortin can influence the time to event (in our case, the time to preterm delivery). The fact that it can be obtained through a blood sample gives it high applicability.
References
- Goldenberg RL, Culhane JF, Iams JD, Romero R (2008) Epidemiology and causes of preterm birth. The Lancet 371(9606): 75-84.
- Challis J, Lye S, Gibb W, Whittle W, Patel F, et al. (2001) Understanding preterm labor. Ann NY Acad Sci 943: 225-234.
- Florio P, Vale W, Petraglia F (2004) Urocortins in human reproduction. Peptides 25(10): 1751-1757.
- Creasy RK, Herron MA (1981) Prevention of preterm birth. Semin Perinatol 5(3): 295-302.
- Florio P, Linton EA, Torricelli M, Faldini E, Reis FM, et al. (2007) Prediction of preterm delivery based on maternal plasma urocortin. J Clin Endocrinol Metab 92(12): 4734-4737.
- Abdullah K, Ebru C, Onder C, Omer Y, Ibrahim H, et al. (2013) Amniotic fluid urocortin-1 concentrations for the prediction of preterm delivery. J Obstet Gynecol 39(7): 1236-1241.
- Iavazzo C, Baka S, Malamitsi-Puchner A (2008) The role of urocortin in gynecological and obstetrical conditions. Arch Gynecol Obstet 279(5): 613-619.
- McLean M, Bisits A, Davies J, Woods R, Lowry P, et al. (1995) A placental clock controlling the length of human pregnancy. Nat Med 1(5): 460- 463.
- Torricelli M, Ignacchiti E, Giovannelli A, MerolaA, Scarpetti E, et al. (2006) Maternal plasma corticotrophin-releasing factor and urocortin levels in post-term pregnancies. Eur J Endocrinol 154(2): 281-285.
- Glynn BP, Wolton A, Rodriguez-Linares B, Phaneuf S, Linton EA (1998) Urocortin in pregnancy. Am J Obstet Gynecol 179(2): 533-539.
