




Meropenem Induced Anaphylactic Shock in a Newborn and Review Of Literature Meropenem
Handan Hakyemez Toptan1, Nilgun Karadag1*, Selahattin Akar1, Tulin Gokmen Yildirim1, Elif Ozalkaya1, MahmutDogru2 and GunerKaratekin1
1Department of Neonatology, ZeynepKamil Maternity and Children’sTraining and Research Hospital, Turkey
2Department of Pediatrics, ZeynepKamil Maternity and Children’s Training and Research Hospital, Turkey
Submission: September 25, 2016; Published: November 10, 2016
*Corresponding author: Nilgun Karadag, Department of Neonatology, ZeynepKamil Maternity and Children’s Research and Training Hospital, Uskudar, Istanbul, Turkey, Tel: +90 216 391 06 80; Fax: +90 216 391 06 90; Email: fbnilg2010@gmail.com
How to cite this article: Handan H T, Nilgun K, Selahattin A, Tulin G Y, Elif O,et al. Meropenem Induced Anaphylactic Shock in a Newborn and Review Of Literature. Acad J Ped Neonatol. 2016; 2(2): 555582. DOI: 10.19080/AJPN.2016.02.555582
Abstract
All drugs have the potential cause to side effects and anaphylaxis.The bioavailability of the drugs is different in newborns. Therefore has the tolerability and efficacy of the medicationsin the newborn period more importance. Meropenem is a broad-spectrum antibiotic used to treat a wide variety of infections. We describe here a neonate who developed anaphylactic shock after use of intravenous meropenem.This is the first reported case of a neonate which develop anaphylactic shock after meropenem administration.
Objectives: To establish normative data for fine motor developmental skills that can be applicable to Egyptian children.
Conclusion: Clinicians should be aware of the potentially fatal adverse effects by use of meropenem in newborns. The rapid intervention of anaphylactic shock saves lives in all age groups.
Keywords: Anaphylactic shock; Meropenem; Newborn
Abbreviations: CRP: C-Reactive Protein; IgE: Immunglobulin E; Min: Minute; NICU: Neonatal Intensive Care Unite; PMNs: Poly Morpho Nuclear leukocytes; TEN: Toxic Epidermal Necrolysis
Introduction
Anaphylaxis is a serious, potentially fatal, systemic allergic reaction that occurs suddenly after contact with an allergic substance and may cause death. The rate of anaphylaxis is increasing yearly, particularly during the first years of life. Newborn infants are less likely to develop anaphylaxis because of their insufficient immune response. Common triggers are foods, medications, and insect stings. All drugs have the potential cause to side effects and anaphylaxis. The global rate of anaphylaxis in the general population is unknown. The prevalence based on international studies varies between 0.05-2% [1]. There is an evidence that these reactions are increasing. Serious adverse drug reactions rose 2.6-fold in the last decades, up to 15% of them have their hospital stay prolonged. About 10% of the general population claim to have a penicillin allergy. It’s difficult to determine the true prevalence, an estimated frequency of penicillin anaphylaxis is reported by 1-5 per 10.000 cases [2].
Penicillin belongs to an important group of antibiotics called beta (ß)-lactam antibiotics. This class of antibiotics includes penicillin and penicillin derivatives such as ampicillin and amoxicillin as well as cephalosporins, monobactams, carbapenems and ß-lactamase inhibitors. Penicillin derivatives can also cause to allergic reactions such as penicillins [3,4]. Newborns are less likely to develop anaphylaxis because of their weak immunoglobulin E (IgE)-mediated immunity and nonimmune mechanisms [2,5]. The true incidence of immunoglobulin (Ig)E-mediated cross-reactivity is not known exactly. Cross-reactivity reactions between penicillins and carbapenems for IgE-mediated are very rare reported [6]. We described here the first case of a newborn who developed anaphylactic shock after administration of intravenous meropenem.
CASE REPORT
A female newborn baby weighing 2690g (10-25th percentile) was born to a 21 years old mother by caesarean section at 36+2 weeks gestation. After birth, she was hospitalized with a diagnosis of polycythemia and transient tachypnea at our neonatal intensive care unit (NICU). Physical examination on admission revealed tachypnea with a heart rate of 158beats/min and respiratory rate of 72/min. The rest of systemic examination, blood pressure measurements and oxygen saturations were in normal range. The baby was kept under warmer with an oxygen replacement of 4L/ min. Arterial blood gas examinations are in normal range. She had a high hematocrit level (69%) at admission, and was treated with intravenous fluid therapy. Blood count and CRP values were also in the normal range.
After four day follow uprising in CRP (5.1mg/dL) values are detected. Meropenem treatment was started after septic work up, but the newborn developed 10 seconds after 20mg/kg intravenous administration of meropenem (Meropenem 500mg/5mL; AstraZeneca Ltd. Şti., Istanbul, Turkey) erythematous rashes and urticaria. The rashes began from the scalp and invaded the entire body in about few minutes (Figure 1). The newborn developed tachypnea, tachycardia and angioedema.Moderate metabolic acidosis (pH: 7.29, pCO2: 52mmHg, pO2: 35mmHg, HCO3: 14mmol/L, base excess: -6mmol/L) and respiratuvar distress was also presented. The blood pressure measurements are hypotensive (before and after meropenem administration the blood pressure was 75/45mmHg, mean 51mmHg; after 29/12mmHg, mean blood pressure 20mmHg, respectively). Prothrombin and activated partial thromboplastin times were within normal range.High-flow oxygen (through mask) was used for respiratory symptoms and hypoxemia at crisis.

The patient was treated with 10cc/kg NaCl 0.9% bolus intravenous fluid infusion in 20 minutes, intramuscularly epinephrine with a dosage of 0.01mg/kg (0.1mL/kg of 1:10.000) and 1mg/kg methylprednisolone. His blood pressure values increased after treatment spontaneously. The rashes began to fade in the first hours, and his blood gases normalized after 60minutes (Figure 2). Investigations showed normal urea, electrolytes, glucose, calcium, magnesium, and liver function tests. The blood tests show a leucocyte count of 8.56x109/L with 56% PMNs and 30% lymphocytes and %8 eosinophilia. Penicillin specific IgE values are elevated (3.5kU/I) and high serum tryptase level 22ng/ mL (2-11.5ng/mL) was observed. Skin tests couldn’t performed at the patient. There was no history of allergy in the medical history. Bloodcultureswere sterile. The patient was discharged after a prolonged hospitalization at the second week of life. The parents are advised to avoid the use of meropenem for any indications and follow-up at child allergy specialist was recommended.
Discussion
We describe here the first case of a newborn who developed anaphylactic shock after intravenous meropenem administration. Meropenem is a broad-spectrum antibiotic used to treat a wide variety of infections. It’s a β-lactam group antibiotic and belongs to the subgroup of carbapenems. The spectrum of meropenem includes many of Gram-positive, Gram-negative and anaerobic bacteria. The mostly observed side effects of this drug are constipation, diarrhea, vomiting, rashes, headache, inflammation at injection site; rarer side effects are apnea, angioedema, erythema multiforme, leukopenia, pleural effusion, Stevens Johnson syndrome, and toxic epidermal necrolysis (TEN) [7]. Meropenem anaphylaxis in newborn is previously not reported. Anaphylactic reactions are rare in newborns because of their weak immunoglobulin E (IgE)-mediated immunity and nonimmune mechanisms [1-3].
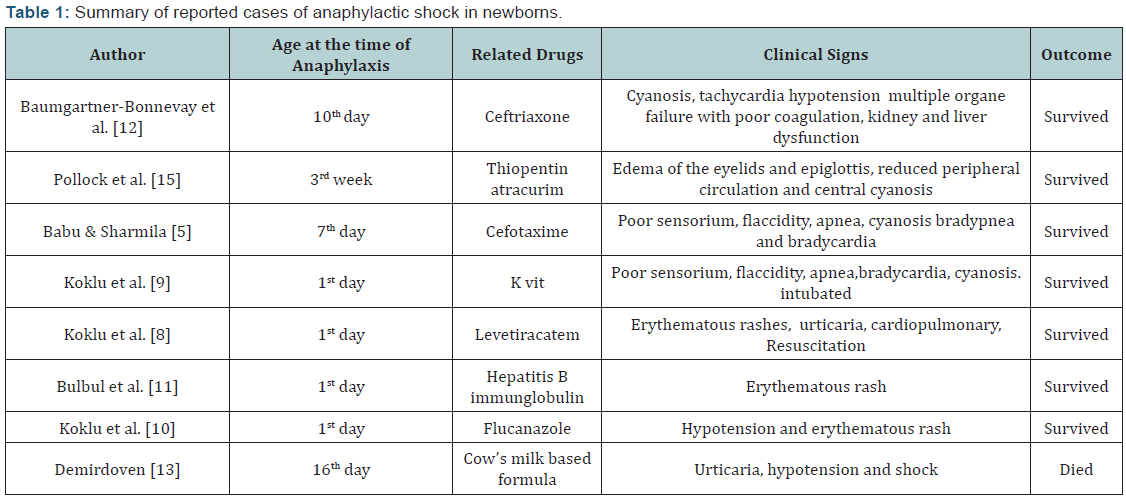
The presentation signs of anaphylaxis in newborns are usually sudden infant death syndrome, poor sensorium, flaccidity, apnea and cyanosis. The majority of anaphylactic reactions involves skin reactions. Other affected organ systems are respiratory, gastrointestinal, cardiovascular and central nervous system. Koklu et al. [8-10] reported three cases of anaphylaxis in the first days of life due to levatiracetam, K vit and flucanazole. Rare cases of anaphylaxis or anaphylactic shock in newborns caused to hepatitis B immunoglobulin, cefotaxime, ceftriaxone, thiopentone, atracurium, flucanazole, K vit and levatiracetam have been also reported. Recently was an anaphylactic shock due to a cow’s milkbased formula in a newborn reported, but all these cases show timely intervention avoid the death in any of these anaphylactic reactions (Table 1) [11-13].
Anaphylaxis is a life-threatening reaction which developed over few seconds-minutes to hours with multisystem involvement. It’s usually triggered by an agent such as food, insect sting, latex or medication, through a mechanism involving immunoglobulin E (IgE), mast cells eosinophils and basophils [1,3]. The diagnosis of anaphylaxis in newborn is difficult because their immune system is immature. Anaphylaxis is a primarily clinical diagnosis, laboratory tests are rarely helpful. There are no tests available in an emergency department to confirm a diagnosis of anaphylaxis in the real time. The diagnosis of anaphylaxis during the acute event is based on clinical presentation and history of a recent exposure to an agent. The tests to find what substance or allergen may trigger the allergic response are usually skin or blood tests. Laboratory tests in serum, plasma, and urine are also helpful in the further diagnosis.
The principal effector cells of systemic anaphylaxis are mast cells and basophils [4,6]. Mediators like tryptase and histamine are released by mast cells and basophils during anaphylaxis. Tryptase is the most abundant secretory granule-derived serine proteinase contained in mast cells and can be used as a marker for mast cell activation. Elevated serum tryptase values are detected in anaphylactic and anaphylactoid reactions, but the negativity cannot exclude the anaphylaxis [1,14]. Blood tests are not sensitive than skin tests, but could be used in patients who are not able to have skin tests. The most common type of blood tests are enzymelinked immunosorbent assay (ELISA, EIA), radioallergosorbent testing (RAST) or immunoassay capture test and blood level of a type of antibody (called immunoglobulin E, or IgE) can help to confirm the diagnose of anaphylaxis. Blood tests revealed elevated tryptase levels in our case too. Anaphylaxis is a clinical emergency, and all healthcare professionals should be able with its recognition and acute and ongoing management. Rapidly intervention has importance in save of lives. Successful management of anaphylaxis is based on early diagnosis and treatment. Epinephrine given intramuscularly remains the mainstay of treatment for this condition. Other second-line therapies, such as inhaled beta-2 agonists, H1 and H2 receptor antagonists and corticosteroids, may play a role in resolving respiratory and cutaneous signs and symptoms [2,4,6]. The symptoms in our patient resolves quickly by administration of epinephrine, antihistamines and steroids. Long-term risk reduction in patients with anaphylaxis focuses on optimal management of relevant comorbidities and relevant immunomodulation [3,14]. We could not found any reports of neonatal anaphylactic shock due to intravenous administration of meropenem in the literature. Our presented case takes attention to anaphylactic shock by use of meropenem in newborns.
Conclusion
Anaphylaxis is a clinical emergency and could be seen in different groups. All healthcare professionals should be able with its recognition and acute and ongoing management. Meropenem is a commonly used broad spectrum antibiotic which could develop fatal anaphylactic reactions in newborns. Clinicians should be aware of the potentially fatal adverse effect by use of intravenous meropenem. The rapid intervention of anaphylactic reactions saves lives in all age groups.
Compliance with Ethical Standards
Funding: This case has been written without support of any found.
Disclosure of Potential Conflicts of Interest
The authors declare they have no conflict of interest.
Informed Consent
Informed consent was obtained from all individual participants included in the case.
Acknowledgement
Hakyemez Toptan H, Karadag N: Writing (all sections), case and review design, editing (introduction, what’s known, what’s new, discussion), revising writing (all sections), Akar S: writing, editing. Dogru M: Child Allergy Specialist, GokmenYildirim T: Writing (all sections), case and review design, editing, Dogru M: Pediatric allergy counseling, Ozalkaya E, Karatekin G: Case design, editing.
References
- Simons FE, Ardusso LR, Bilò MB, El-Gamal YM, Ledford DK, et al. (2011) World allergy organization guidelines for the assessment and management of anaphylaxis. World Allergy Organ J 4(2): 13-37.
- Simons FE, Ardusso LR, Bilò MB, Cardona V, Ebisawa M, et al. (2014) International consensus on (ICON) anaphylaxis. World Allergy Organ J 7(1): 9.
- Albin S, Agarwal S (2014) Prevalence and characteristics of reported penicillin allergy in an urban outpatient adult population. Allergy Asthma Proc 35(6): 489-494.
- Moore TJ, Cohen MR, Furberg CD (2007) Serious adverse drug events reported to the Food and Drug Administration, 1998-2005. Archives of Internal Medicine. 167(16): 1752-1759.
- Babu TA, Sharmila V (2011) Cefotaxime-induced near-fatal anaphylaxis in a neonate: a case report and review of literature. Indian J Pharmacol 43(5): 611-612.
- Kula B, Djordjevic G, Robinson JL (2014) A systematic review: can one prescribe carbapenems to patients with IgE-mediated allergy to penicillins or cephalosporins? Clin Infect Dis 59(8): 1113-1122.
- Zhanel GG, Wiebe R, Dilay L, Thomson K, Rubinstein E, et al. (2007) Comparative review of the carbapenems. Drugs 67(7): 1027-1052.
- Koklu E, Ariguloglu EA, Koklu S (2014) Levetiracetam-induced anaphylaxis in a neonate. Pediatr Neurol 50(2): 192-194.
- Koklu E, Taskale T, Koklu S, Ariguloglu EA (2014) Anaphylactic shock due to vitamin K in a newborn and review of literature. J Matern Fetal Neonatal Med 27(11): 1180-1181.
- Koklu E, Kalay S, Koklu S, Ariguloglu EA (2014) Fluconazole administration leading to anaphylactic shock in a preterm newborn. Neonatal Netw 33(2): 83-85.
- Bulbul A, Karadag A, Köklü E, Pamuk U, Sarici SU (2010) Anaphylactic shock due to hepatitis B immunoglobulin in a newborn. J Matern Fetal Neonatal Med 23(10): 1257-1259.
- Baumgartner-Bonnevay C, Choquet-Kastylevsky G, Putet G, Bleyzac N, Vial T, et al. (2002) Anaphylactic shock associated with ceftriaxone therapy in a newborn. Arch Pediatr 9(10): 1050-1052.
- Demirdöven M, Keleş E, Gebeşçe A, Yazgan H, Kaya M, et al. (2015) Anaphylactic shock due to cow’s milk allergy in the neonatal period. Breastfeed Med 10(6): 341.
- De Schryver S, Halbrich M, Clarke A, La Vieille S, Eisman H, et al. (2016) Tryptase levels in children presenting with anaphylaxis: Temporal trends and associated factors. J Allergy ClinImmunol 137(4): 1138- 1142.
- Pollock EM, MacLeod AD, McNicol LR (1986) Anaphylactoid reaction complicating neonatal anaesthesia. Anaesthesia 41(2): 178-180.















