




Case Report
Congenital-Infantile Fibro sarcoma of Hand – A Case Report
Dinesh Prasad Koirala*, A.K.M Zahid Hossain1, Gazi Zahirul Hasan2 and Md. Tossaddeque Hossain Siddiqui3
Department of Paediatric Surgery, Bangabandhu Sheikh Mujib Medical University, Bangladesh
Submission: May 25, 2016; Published: June 24, 2016
*Corresponding author: Dinesh Prasad Koirala, Department of Paediatric Surgery, Bangabandhu Sheikh Mujib Medical University, Bangladesh; Email: koiraladinesh1@hotmail.com
How to cite this article: YDinesh P K, A.K.M Zahid H, Gazi Z H, Md. Congenital-Infantile Fibro sarcoma of Hand – A Case Report. Acad J Ped Neonatol. 2016; 1(2): 555560. DOI: 10.19080/AJPN.2016.01.555560
Abstract
Congenital infantile fibro sarcoma is a rare malignant tumor of the soft tissue in the infant primarily developed in the soft tissue of distal extremities and occasionally in unusual location such as the lungs and retro peritoneum. It occurs mainly in children below the age of 5 years. About 250 cases have been reported in the literature so far, very few of them in newborns. Its clinical course differs from conventional fibro sarcoma, the prognosis is relatively good compared to adult forms and the 5 year survival rate can be more than 80%. We report a case of congenital infantile fibro sarcoma of the hand treated successfully by below elbow amputation. The child is now 5 years old with no recurrence.
Keywords: Fibro Sarcoma; Congenital; Infantile
Introduction
Congenital infantile fibro sarcoma is an uncommon soft tissue malignancy. It usually affects the extremities [1]. Few cases involving the hand were reported and a limited number were presents during neonatal period. It represents less than 1% of all childhood malignancy, but it is the most common soft tissue sarcoma in less than 1 year of age. Clinically there may be rapid growth of the tumor so the initial clinical diagnosis is often erroneous [2]. Although histological similar to fibro sarcomas occurring in adults, congenital-infantile fibro sarcomas differs in their clinical behavior, metastasis is rare and local recurrence is common. The prognosis is good, much better than that for histological similar fibro sarcoma seen in adults. In one series the 5 year survival rate for congenital-infantile fibro sarcoma was more than 80%, which is in sharp contrast to fibro sarcoma in adults, where 5 year survival rate is only 35% [3]. We report a case of congenital infantile fibro sarcoma involving the left hand in a 25 days old male infant, managed by forearm amputation and followed up for 5 years without recurrence or metastasis.
Case Report
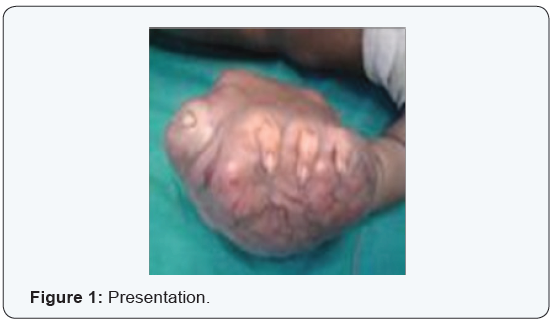
A 25 days old baby present with painless swelling of the left hand. Parents had noticed a nodule on the palm of the left hand since birth, which enlarged rapidly. The child was treated with different antibiotic and homeopathic medicine locally. Because of rapid enlargement of the swelling, the child was referred to our hospital when he was about 1 month old. On physical examination he was a normal healthy baby of 3 kg weight and a mass in the left hand which was poorly circumcised, measuring about 8cm x 8cm, firm in consistency, skin was tense and shiny. Other physical examination reveal no abnormality.
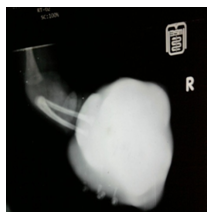
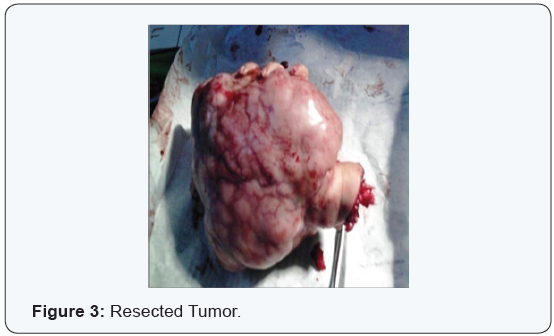
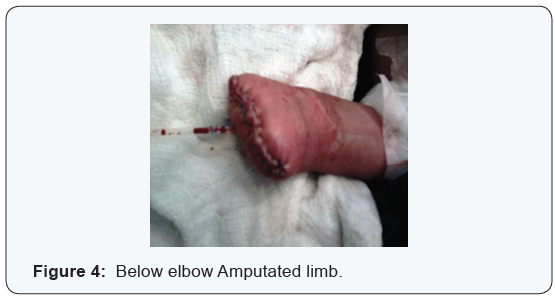
Plain x-ray of the left hand showed a huge soft tissue mass. The laboratory tests, x-ray chest, abdominal Ultrasonography was normal. Fine needle aspiration cytology (FNAC) of the mass was done. It showed malignant spindle cell tumor. The size of tumor was rapidly increasing doubling its size within 2 weeks. Open biopsy was done which suggested soft tissue sarcoma. The management was an below elbow amputation and his to pathological examination confirmed the diagnosis. Gross pathological specimen showed skin with underlying tumor tissue which infiltrating fat, skeletal muscle, bone and neuro-vascular bundle. It was not involving the respected margins. Cut surface was gray white with area of necrosis. Microscopic examination confirmed features of infantile fibro sarcoma with Herring bone pattern. Postoperatively the baby was stable. The child was followed up for 5 years of age without evidence of recurrence or metastasis.
Discussion
The congenital infantile fibro sarcoma is a rare soft tissue malignant tumor. Fibro sarcoma is primarily an adult malignancy and histological similar to those seen in children. The congenital infantile fibro sarcoma usually occurs at birth or in the neonatal period, mostly presenting within the first six months of life [4]. No significant sex predilection has been found [3].
These tumors originate from the primitive mesenchymal tissue. There is no evidence of increased familial incidence but a recent study showed that all patients with congenital infantile fibro sarcoma under the age of two years exhibited some type of chro mosomal gain. Most had trilogies of chromosome 8, 11, 17 and/or 20 and an abnormal karyotype 48 xy, 11 and 20 [5,6].
Clinically, they present with a rapidly enlarging swelling in the soft tissue most commonly in the extremities (71%) but may present axial locations (29%) as well. When the limbs are involved, the tumor tends to affect the leg more than the arm and the distal extremity more than the proximal one [1]. A limited number however developed primarily in the bones [7]. Therefore the initial clinical diagnosis is often erroneous [2]. The diagnosis is sometimes made base on a fast growing soft tissue swelling. At times it is discovered late before one year [8]. On plain x-ray showed soft tissue swelling that may obliterate normal fat planes and deform or destroy the adjacent bone. CT scan is useful in demonstrating the extent of the tumor and the amount of bony involvement, where as MRI is particularly useful in showing the disruption of the soft tissue planes. The MRI findings of congenital infantile fibro sarcoma usually include a mixed cystic and solid tumor of heterogeneous density which typically has in homogenous enhancement [6]. Although the imaging findings are non specific, congenital infantile fibro sarcoma should also be considered in cases of a soft tissue mass in infants. A biopsy should be done to avoid delayed and incorrect management [9].
Antenatal and postnatal ultrasound usually shows a poorly circumscribed, heterogeneous and vascularize soft tissue mass, which grows very rapidly and cause deformity of the anatomical region involved, sometimes it causes polyhydramnios. Rest of the fetus is usually normal. The diagnosis is done by the histological examination having an plastic spindle shaped cells arranged in a herring bone pattern, however, some of the striking features are uniform, well oriented fibroblast, scattered round cells and chronic inflammatory cells like lymphocytes. Multinucleated giant cells are rare. Mitotic figures are common features. Rich vascular areas may be seen [10].
Although histological similar to fibro sarcoma in adults, congenital- infantile fibro sarcoma differs in its clinical behavior compared with the adult type. Metastases are rare, however, local recurrence is common. The prognosis for congenital-infantile fibro sarcoma is extremely good with a 5 year survival rate of 84% in series of 53 cases [2]. Treatment is wide local excision or amputation. Chemotherapy and radiotherapy are reserved for unrespectable tumor and for recurrence or metastasis. Amputation is indicated only in the cases of local recurrence, giant tumor involving bone and neurovascular structures [8].
Conclusion
In the case of our child the presence of diffuse soft tissue involvement of the hand and the bony lesions incite us to do a biopsy which revealed a well differentiated congenital fibro sarcoma. The extent of the tumor growth made us to perform an below elbow amputation of the hand. That gave us a good result because no metastasis or local recurrence were noted after 3 years however follow up should be longer to look for these evolution aspects [11]. There are high metastatic and mortality rate for axial lesions, indicating a more aggressive behaviors. The relatively benign course of such tumors may be due to a significantly lower proliferative index coupled with enhanced apoptosis. The favorable clinical course and biological features of congenital-infantile fibro sarcomas have raised a question about its nomenclature as sarcoma rather than a borderline tumor [5,10].
Summary
In summary, although congenital-infantile fibro sarcoma is a rare soft tissue tumor in children, it should be included in the differential diagnosis of a large extremity mass presenting at birth because the prognosis is much better than adult type. CT provides the information about bony involvement but shows poor demarcation of the extent of the tumor. On the other hand, MRI is particularly useful in delineating the extent of the tumor. It also provides multilane views so that diagnosis and planning for treatment can be reinforced (Figures 1-4).
References
- Blocker S, Koenig J, Ternberg J (1987) Congenital Fibro sarcoma .J pediatric surge 22(7): 665-670.
- Chung EB, Enginger FM (1976) Infantile Fibro sarcoma. Cancer 38: 729-739.
- Vinnicombe SJ, hall CM (1994) Infantile fibro sarcoma; radiological and clinical features, Skeletal Radiology 23(5): 337-341.
- Lee Mj , Cairns RA, Munk PL, Poon PY (1964) congenital infantile fibro sarcoma ;magnetic resonance imaging findings. Can association Radiol J 47(2):121-125.
- Wilson MB, Stanley W, Sens D, Garvin AJ (1990) infantile Fibro sarcomaa misnomer? Paed pathology 10(6): 901-907.
- Pousti JJ, Upton J, Loh M (1998) Congenital fibro sarcoma of the upper extremity. plast Reconstruction Surg 102(4): 1158-1162.
- Dahlin DC (1982) infantile Fibro sarcoma, Skeletal Radiol 8(1): 77-78.
- Sah SP, Agrawal CS, Rani S (2000) Congenital infantile fibro sarcoma of the upper extremity, Indian J pathology Microbiol 43(3): 347-349.
- Cheng SM, Shih SL, shen CY (1999) congenital –infantile fibro-sarcoma: A case report chin J radiol 24(3): 137-139.
- Chetan G, Bhat V, Sreerag K.S, Jagdish S, Jayanthis (2008) Congenital Fibro sarcoma Of Foot-A case report, Current Pediatric 12(1&2): 9-11.
- Ngom G, Dieme C, Fall M, San Kale AA , Fall, et al. (2006)Congenital Hand Fibro sarcoma in Child. J Orthopaedics 3(4): 19.















