




Experience and Knowledge of Female Genital Mutilation amongst London Obstetrics and Gynaecology Trainees
Ka Ying Bonnie Ng1,2* and Balvinder Sagoo3
1Department of Obstetrics and Gynaecology, Chelsea and Westminster Hospital, UK
2Academic Department of Obstetrics and Gynaecology, Princess Anne Hospital, UK
3Department of Obstetrics & Gynaecology, London North West Healthcare NHS Trust, UK
Submission: April 14, 2016; Published: May 02, 2016
*Corresponding author: Ka Ying Bonnie Ng, Academic Department of Obstetrics and Gynaecology, Princess Anne Hospital, Coxford Road, Southampton, SO16 5YA, UK; Email: bonnie.ng@doctors.org.uk
How to cite this article: RNg KYB, Sagoo B. Experience and Knowledge of Female Genital Mutilation amongst London Obstetrics and Gynaecology Trainees. J Gynecol Women’s Health. 2016; 1(2): 555557. DOI: 10.19080/JGWH.2016.01.555557
Abstract
Our aim was to explore the knowledge and experiences of London Obstetrics and Gynaecology (O&G) trainees. An online questionnaire was designed and distributed to London O&G trainees to assess their knowledge and experiences of FGM. The questionnaire was distributed to 108 trainees, and 33 responses were obtained (response rate of 30.6 %). 84.9% were comfortable with talking to a patient about FGM, 75.8% reported that majority of patients do not volunteer information about their FGM. The significant barriers to communication were language and culture. Although most trainees (84.9%) could describe the 4 types of FGM, 42.4% had never attended FGM teaching. 72.7% knew how to refer patients to FGM services and only 42.4% were aware of FGM support groups. Focused training in FGM for O&G trainees may increase confidence, knowledge of support available and referral systems to improve quality of care for patients suffering from FGM.
Keywords: Female genital mutilation; Infundibulation; Cutting; Obstetric and gynaecology training; Learning; Communication
Conclusion: FGM: Female Genital Mutilation; O&G: Obstetrics and Gynaecology; WHO: World Health Organization
Introduction
The World Health Organization (WHO) estimates that 140 million women worldwide have undergone some form of female genital mutilation (FGM) [1]. Approximately 91.5 million girls and women above 9 years old are currently living with consequences of FGM, with an estimated 3 million at risk of undergoing FGM every year [1]. The problem is concentrated in Africa and middle-eastern countries, but with migration, prevalence is increasing in high-income countries. FGM in the UK is amongst those in migrant communities and annually over 20, 000 girls under 15 years of age are at risk [2]. FGM breaches international human rights law, the United Nations Convention on the Rights of the Child [3] and is a criminal offence in many areas of the world. In the UK, under the Female Genital Mutilation Act 2003, it is illegal to infibulate or mutilates the whole, or any part of a girl’s labia minor or clitoris, whether in the UK or overseas.
There are four classes of FGM: type 1 is removal of clitoris or prepuce; type 2 is removal of the clitoris and the labia minora; type 3, ‘infundibulation’, is the narrowing of the vaginal orifice; type 4 includes other harmful procedures to female genitalia for non-medical purposes [4]. FGM can lead to serious consequences, including infection and haemorrhage in the short-term. In the long-term, there may be post-traumatic stress disorder and depression, as well as difficulties with urination, menstruation and sexual intercourse, and numerous other gynaecological and obstetric problems [5,6]. Despite significant negative consequences, members from affected communities continue to support FGM, associating it with their female sexuality and culture [7]. The RCOG green top guidelines emphasize that healthcare workers should actively demonstrate knowledge and respect, be familiar with the complications of FGM, and that patients should be recognized and appropriately counseled [8]. There is also a duty of healthcare professionals to report all ‘known’ cases of FGM in under-18s which they identify in the course of their professional work, to the police [9].
With increasing prevalence of FGM in the UK and clinical duties to recognise FGM affected patients, we wanted to assess the knowledge and experience of FGM of obstetrics and gynecology trainees in London, where there is a high risk population. We aimed to establish a trainee’s confidence, and potential barriers, in talking to patients with FGM, their knowledge of FGM and services available to patients and finally their education on the subject.
Materials and Methods
An online questionnaire was designed and distributed to 108 London obstetrics and gynaecology trainees to assess their knowledge and experiences of FGM in February 2015 (appendix). Trainees were identified from the London School of Obstetrics and Gynaecology trainees register. An email was sent out to London obstetric and gynaecology trainees through the London School of Obstetrics and Gynaecology with a link to the online questionnaire. Survey Monkey was used for questionnaire design. Participation in the study was entirely voluntary, anonymous, and the site did not allow respondents to submit more than one questionnaire.
Trainee’s experience of FGM was assessed by asking them whether they were comfortable talking about FGM to their patients, whether patients volunteered information about their FGM, the main complications of FGM seen in clinical practice and factors that made consultation with FGM patients difficult. Trainee’s knowledge and training in FGM practice was assessed by asking them whether they were able to describe the types of FGM practice, whether they had attended any local or national teaching in FGM, how often the topic of FGM was raised in their workplace, whether they were aware of FGM support groups available, whether they know their nominated FGM consultant or specialist nurse and whether they know how to refer to FGM services. The results from Survey Monkey were collected and analyzed by two independent researchers.
Results
The questionnaire was distributed to 108 London trainees, and 33 were completed and returned (response rate of 30.6%). Amongst our cohort, the mean duration O&G experience was 5.2 years (range 1-14 years). The trainees were training at St Mary’s Hospital (9/33 trainees, 23.3% of cohort), West Middlesex Hospital (8/33, 24.2%), Chelsea and Westminster Hospital (7/33, 21.2%), Queen Charlotte’s Hospital (3/33, 9.1%), Northwick Park Hospital (3/33, 9.1%), Hillingdon Hospital (1/33, 3%) and Ealing Hospital (1/33, 3%).
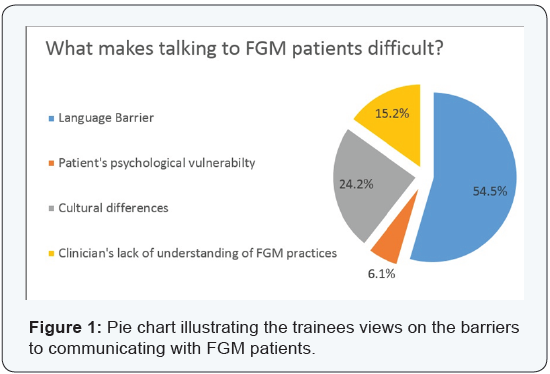
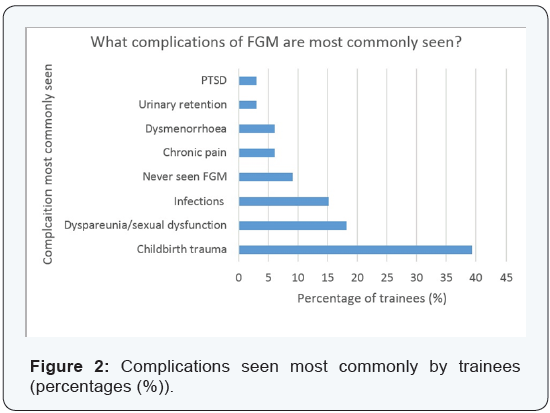
On assessing whether trainees were comfortable with talking about FGM to their patients, the majority (16/33, 48.5%) felt ‘quite comfortable’, 36.4% felt ‘very comfortable’, 9.1% were ‘not comfortable’ and 6.1% were ‘not at all comfortable’. Over three quarters (75.8%) of trainees said that FGM patients will not volunteer information about their condition. Trainees identified four main factors that contribute to difficulties when talking to patients with FGM; these were language barriers (54.5% of trainees), cultural differences (24.2%), their own lack of clinical understanding of FGM (15.2%) and patient’s psychological vulnerability (6.1%) (Figure 1). The complications of FGM most commonly seen by trainees are childbirth trauma (reported by 39.4% of trainees), sexual dysfunction and dyspareunia (18.2%), infections (15.2%), dysmenorrhoea (6.1%), PTSD (3%), urinaryretention (3%). 3 out of 33 London trainees (9.1%) had not encountered a case of FGM in their training (Figure 2).
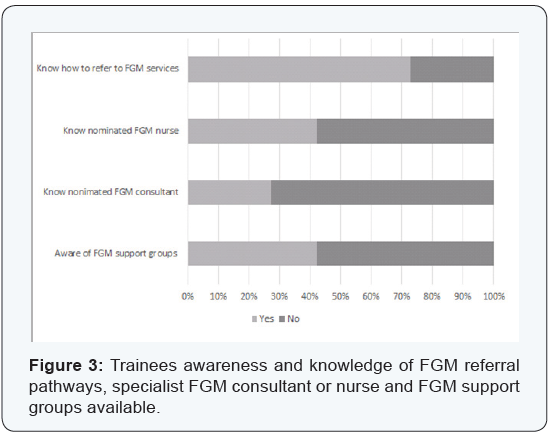
The majority of trainees reported that they were able to report all four types of FGM practice (28/33 trainees, 84.9%). 57.6% of trainees (19/33) had attended some form of FGM training, either at a local or national level. Figure 3 shows the trainee’s knowledge of support groups and specialist services available to FGM patients. Less than half of the trainees (14/33, 42.4%) were aware of support groups available for woman affected by FGM. Only 27.3% (9/33) and 42.4% (14/33) knew whether there was a nominated FGM consultant or specialist nurse respectively. 72.7% (24/33) of trainees knew how to refer patients to FGM services. The topic of FGM is raised in the workplace most commonly once a month (57.6% of trainees), followed by once a week (36.4%).
Discussion
Main findings
Our study suggests that majority of obstetrics and gynaecology trainees in London are comfortable with discussing FGM with their patients. However, there are many barriers to discussing FGM with patients; over 75% of trainees reported that these patients do not volunteer information. The difference in language and culture are highlighted as significant barriers to communication in these patients. Lack of clinical understanding of FGM and also a patient’s psychological vulnerability were noted to be relevant too. This study also identified lack of training and education in FGM, illustrated by less than 60% of trainees in our cohort having had some form of local or national training. Less than half of trainees were aware of support groups available for patients affected by FGM. Focused training in the area of FGM amongst O&G trainees may increase confidence, knowledge of support available and referral systems for patients suffering from FGM.
Strengths
This observational study has been performed in London, addressing a trainee cohort that is likely to have a higher exposure to FGM patients relative to some other training areas in the UK. The lack of trainee education and training in FGM highlighted by our trainee cohort is therefore particularly important in London’s multicultural community. Our study used a simple anonymous questionnaire, which allowed submission of one questionnaire from each participant only, avoiding duplication of results. The anonymous nature of the study encouraged the trainees to be honest in their responses. Online submission of the questionnaire was convenient and allowed easy and accurate data collection.
Limitations
Although the questionnaire was distributed to 108 London obstetrics and gynaecology trainees via an email link, only 33 responded, giving a response rate of just over 30%. This means that the findings may not be representative of the whole trainee cohort in London. Although not done, due to small study numbers, subgroup analysis to identify effects of years of O&G experience, trainee level and type of hospital, would have been useful. The study was only performed in one centre, reducing the applicability of our findings in other training areas across the UK. Although this was a small study, the findings still illustrate exposure of FGM to London trainees and that their knowledge and confidence may be significantly improved through focused training in this area.
Interpretation
Although FGM is performed in high risk communities, including Africa, Asia and the Middle East, increasing migration means that women who have been affected by FGM are increasingly found in the UK. An estimated 137, 000 women and girls (including 10 000 girls aged under 15) in England and Wales have undergone FGM [8]. London has the highest prevalence rate in England and Wales; an estimated 2.1% of women are affected by FGM [10]. FGM refers to ‘all procedures involving partial or total removal of the female external genitalia for non-medical reasons’. Community base prevention work has allowed us to establish the reasons behind why woman continue to practice FGM, even when they have migrated to the UK; some still support FGM, linking it to their culture and/or control of their female sexuality [7].
The RCOG highlights in their revised guidelines (July 2015) [8] that clinical management of women with FGM requires high quality of care that is accessible, sensitive and informed [8]. Recently, the UK law states that it is a requirement for trainees to report any girl under the age of 18 with confirmed FGM (either by examination or because the parent or patient says that it has been done) to the police within one month of confirmation [8]. Such guidance set by the royal college illustrates the importance of increased focused training and education, to improve confidence and knowledge in a highly sensitive discussion topic. Appropriate communication and addressing important barriers to talking to FGM patients is paramount, and is especially important given that a significant proportion of patients affected will not voice their condition voluntarily. Trainees reported that childbirth trauma is the most commonly seen complication of FGM in clinical practice. Women affected by FGM are 3.3 times more likely to experience a difficult labour and 2 times more likely to have an obstetric haemorrhage [11]; they are more likely to have obstetric lacerations, instrumental deliveries and inelastic scar tissue may cause obstruction and prolong labour [12]. However, in the long term, FGM affected patients have an extensive list of potential complications, many of which were not identified by the trainees in our cohort, including post-traumatic stress disorder and depression, difficulties with urination, menstruation and sexual intercourse, and numerous other gynaecological and obstetric problems [5,6].
There are some online e-learning resources developed to increase awareness of FGM amongst the public sector workforce. An online FGM training package has been launched by the Home Office, which is aimed at educating professionals who will come into contact with girls as risk of FGM; this includes teachers, police, doctors, social workers and Border Force staff [13]. In addition, Health Education England offers an online learning resource through the ‘e-learning for Healthcare’ scheme, that includes modules on issues surrounding FGM, communication skills for FGM consultations and legal and safeguarding issues regarding FGM in the UK [14]. Although there are online e-learning resources available, it is unclear whether trainees engage or benefit from them. Almost 85% of trainees self-reported that they could describe all four types of FGM, so knowledge may be sound. However, less than 60% of trainees in our cohort had attended any form of FGM training locally or nationally. Perhaps focused FGM courses or ‘study days’ may be better attended and better received by trainees and will more likely address communication barriers and consultation skills with FGM patients. For example, although ‘FGM’ is understood by and accepted by some women, trainees will need to appreciate that some woman may find words such as ‘closed’, ‘cut’, or ‘circumcised’ more suitable [15]. Trainees also need to be familiar with the process of reporting FGM and be able to explain to woman its purpose.
It is also clear from our study that a significant proportion of trainees did not know whether they had a designated FGM consultant or specialist nurse, and there is still a significant gap in the knowledge of referral pathways for FGM patients.
Conclusion
Although obstetric and gynaecology trainees are mostly confident in discussing FGM with patients, there are still some significant barriers to communication, namely differences in culture and language. Our study highlights the need for focused education and training in the area of FGM, including emphasis on communication and consultation with patients, raising awareness of available support groups, as well as local guidance on the specialist referral of FGM patients. The prevalence of FGM in the UK is increasing and every trainee is responsible for identifying cases where there has been a violation of human rights in vulnerable women. Trainees should have the knowledge and training to enable the delivery of high quality care to those affected by FGM, addressing long term psychological and physical complications.
Contribution to Authorship
Study concept and design was by Ka Ying Bonnie Ng. Data analysis, data interpretation and manuscript development was by Ka Ying Bonnie Ng and Balvinder Sagoo.
References
- World Health Organisation (WHO) (2015) Sexual and Reproductive Health. Female genital mutilation and other harmful practices, Switzerland.
- Gov UK (2015) Female genital mutilation the facts.
- UNICEF (2014) Fact sheet: a summary of the rights under the Convention on the Rights of the Child.
- World Health Organisation (WHO) (2015) Sexual and reproductive health. Classification of female genital mutilation.
- Banks E, Meirik O, Farley T, Akande O, Bathija H, et al. (2006) Female genital mutilation and obstetric outcome: WHO collaborative prospective study in six African countries. Lancet 367(9525): 1835- 1841.
- Brown K, Beecham D, Barrett H (2013) The Applicability of Behaviour Change in Intervention Programmes Targeted at Ending Female Genital Mutilation in the EU: Integrating Social Cognitive and Community Level Approaches. Obstet Gynecol Int 2013: 324362.
- The Royal College of Obstetricians and Gynaecologists (RCOG) (2015) Green-top guideline No. 53: Female Genital Mutilation and its Management.
- Gov.Uk Home Office And Department of Education (2015) Mandatory reporting of Female Genital Mutilation- procedureal information.
- Gov UK (2015) Female Genital Mutilation: Resource Pack.
- Berg RC, Underland V (2013) The obstetric consequences of female genital mutilation/cutting: a systematic review and meta-analysis. Obstet Gynecol Int 2013: 496564.
- Browning A, Allsworth JE, WALL LL (2010) The relationship between female genital cutting and obstetric fistulae. Obstet Gynecol 115(3): 578-583.
- The Home office (2015) Free online training for frontline professionals in helping girls at risk of FGM.
- health Education England (2015) e-learning for Healthcare: Female genital mutilation.
- Hm Governement (2014) Multi-agency Practice Guidelines: female genital mutilation. London, UK.
